

The Osseotransportation Techniques in Sinus Lifting
The posterior maxilla presents a unique challenge in implant dentistry due to reduced bone height, compromised bone quality, and the proximity of the maxillary sinus. For decades, clinicians have used bone graft materials to augment this area before or during implant placement. However, evolving scientific evidence has introduced an alternative biologically driven strategy: the osseotransportation concept in sinus lifting. This approach emphasizes the body’s innate capacity for bone regeneration by creating and maintaining space beneath the elevated Schneiderian membrane without relying on large volumes of graft material.
This article explores the biological basis, clinical application, outcomes, and practical considerations of osseotransportation in sinus lifting, providing dental professionals with a comprehensive understanding of this evolving technique.
Understanding Osseotransportation in Sinus Lifting
The osseotransportation concept refers to the coordinated process by which bone is generated in the sinus cavity following elevation of the sinus membrane. Conventionally, sinus lifting has involved grafting with autogenous bone, allografts, xenografts, or synthetic substitutes to fill the space created between the sinus floor and the Schneiderian membrane. In contrast, osseotransportation relies on the body’s biological mechanisms to form bone once space is created and stabilized.
The premise is straightforward: space creation is the precursor to bone regeneration. When the sinus membrane is elevated and the created space is maintained — whether by the implant itself, specialized devices, or careful surgical manipulation — a stable blood clot forms. This blood clot, in combination with osteoprogenitor cells and growth factors from the surrounding bone and the membrane, becomes the scaffold for new bone formation. The osseotransportation concept aligns with key biological principles such as mechanotransduction and Wolff’s law, which underscore how functional loading and controlled space maintenance influence bone remodeling and growth.
Biological Basis Behind Osseotransportation and Bone Regeneration
At the core of the osseotransportation concept in sinus lifting is the biological activity of the Schneiderian membrane and the native bone. The Schneiderian membrane is not a passive lining; it contains cells capable of expressing osteogenic markers — indicating its potential to participate in bone formation. When elevated, this membrane contributes osteoprogenitor cells and biologically active signaling to the regenerative process.
Once the membrane is lifted, the resultant compartment is initially filled with a blood clot. This clot serves as a natural provisional matrix that supports the migration of mesenchymal stem cells and vascular ingrowth. The adjacent alveolar bone and lateral sinus walls provide sources of osteogenic cells that populate the space. Over time, these cells differentiate and deposit bone matrix, gradually transforming the space into mineralized bone.
This biological foundation shifts the paradigm from “filling” with bone substitutes to “facilitating” bone growth by maintaining a stable space under the membrane. It underscores why osseotransportation is increasingly embraced for cases where residual bone height is moderate and predictable bone gain is feasible.
Clinical Techniques and Protocols for Osseotransportation in Sinus Lifting
Several surgical techniques leverage the osseotransportation concept, and each aims to maintain the elevated sinus membrane and encourage native bone formation:
1- Indirect Sinus Lift (Osteotome Technique)
The indirect sinus lift, commonly performed using the osteotome technique, is a minimally invasive approach that allows elevation of the sinus floor through the crestal aspect of the alveolar ridge. Using specially designed osteotomes, the clinician carefully fractures and displaces the sinus floor upward, creating a space between the residual bone and the Schneiderian membrane. The space is naturally filled with a blood clot, which acts as a scaffold for bone regeneration. In many cases, the dental implant is placed simultaneously, with its apex helping to maintain the elevated space. This technique is particularly effective for patients with moderate residual bone height and offers reduced surgical morbidity compared to lateral approaches, while leveraging the body’s innate regenerative capacity for predictable bone formation.
2- Direct Lateral Window Approach Without Grafts
The direct lateral window sinus lift is indicated in cases with more pronounced bone deficiency, where the residual alveolar height may not be sufficient for an indirect approach. A small lateral window is created in the lateral wall of the maxillary sinus, allowing direct access to elevate the Schneiderian membrane carefully. Instead of introducing bone graft material, the elevated space relies on the stability of the membrane and the formation of a blood clot to induce new bone growth. This technique maximizes the regenerative potential of the sinus environment, reduces complications associated with graft materials, and allows simultaneous or delayed implant placement depending on primary stability and surgical considerations. Proper membrane handling and space maintenance are essential to achieve successful outcomes with this graftless approach.
3- Hydraulic and Balloon Elevation Techniques
Hydraulic and balloon sinus elevation techniques are modern alternatives to traditional sinus lifts, emphasizing atraumatic and controlled elevation of the Schneiderian membrane. Using either carefully controlled hydraulic pressure or small inflatable balloon devices, the sinus membrane is gently lifted to create the desired vertical space. Once elevated, the space is maintained by the implant itself or specialized tenting devices to support bone formation. These techniques reduce the risk of membrane perforation and patient morbidity, while promoting natural bone regeneration without the need for graft materials. Hydraulic and balloon methods are particularly beneficial in cases where precision and minimally invasive approaches are desired, offering predictable vertical bone gain and high implant success rates.
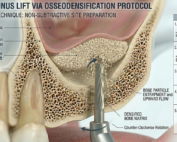
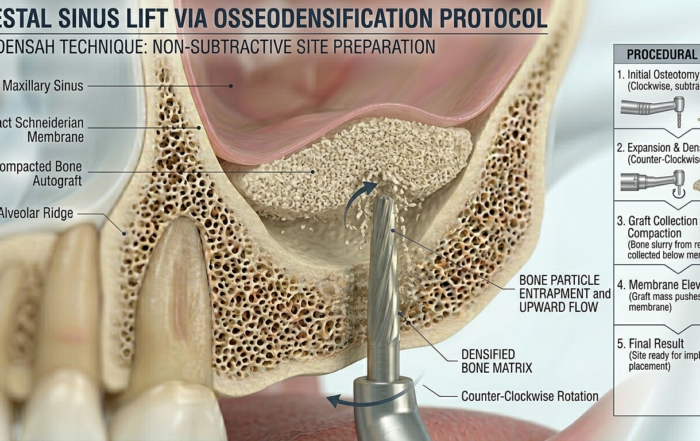
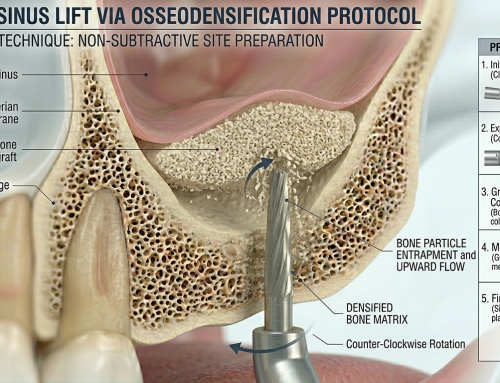
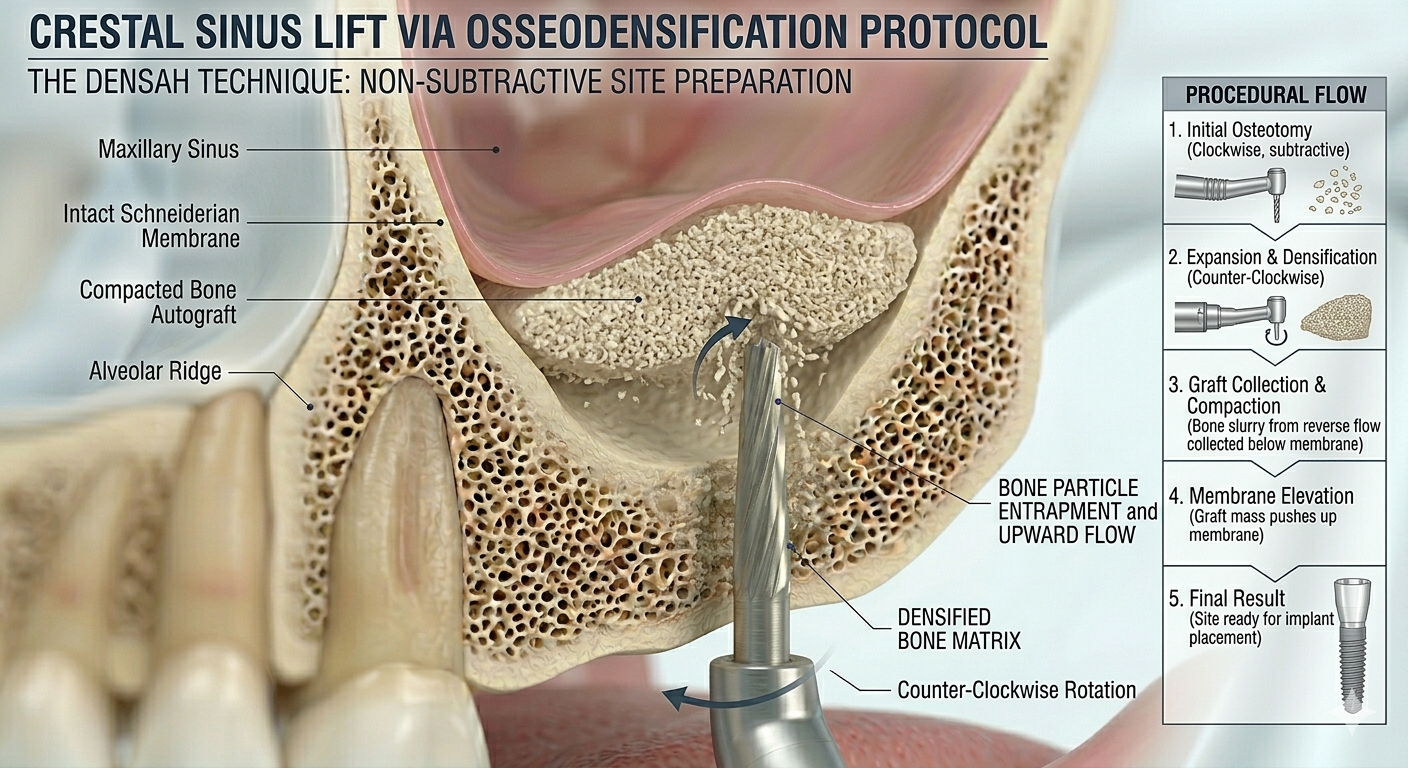
4- Osseodensification‑Assisted Sinus Lift
Osseodensification-assisted sinus lifts utilize specially designed drills that compact, rather than remove, bone during preparation of the osteotomy site. This compaction increases bone density and simultaneously elevates the sinus membrane, creating a stable space for bone regeneration. By enhancing the primary stability of the implant and maintaining the sinus elevation, this technique leverages both mechanical and biological principles to support bone formation without graft materials. Osseodensification is particularly advantageous in patients with low to moderate residual bone height, where conventional drilling might compromise bone integrity. The technique also improves implant stability, reduces micromovement, and creates an environment conducive to predictable osseointegration in graftless sinus augmentation procedures.
Across all techniques, the clinician’s skill in membrane management, atraumatic elevation, and space maintenance is critical. Avoiding membrane tears and ensuring primary implant stability are prerequisites for predictable outcomes.
5- Sinus Lift Implant (SinusFuse): Achieving More With Less
SinusFuse is an advanced dental implant engineered to function simultaneously as a sinus lift instrument and a definitive implant, redefining efficiency in posterior maxillary rehabilitation. Its patented apical blades are specifically designed to gently up-fracture the sinus floor while minimizing the risk of Schneiderian membrane perforation. A unique reverse helical side-cut geometry allows autogenous bone to be shaved during insertion and immediately transported internally toward the elevated sinus space. These bone particles are preserved within a concave, dish-shaped apical reservoir, enabling controlled osseotransportation without external exposure or contamination. By harvesting, transporting, and stabilizing the patient’s own bone in a single step, SinusFuse achieves predictable sinus elevation and bone regeneration with reduced surgical complexity and biological compromise.
Interested in knowing more about Sinusfuse? Read the article :
Clinical Outcomes, Bone Gain, and Implant Survival
A substantial body of clinical evidence supports the effectiveness of osseotransportation in sinus lifting. Multiple studies demonstrate that adequate vertical bone gain and high implant survival rates can be achieved without the use of bone grafts.
For indirect sinus lift procedures performed without graft material, studies have reported average vertical bone gains of approximately 2 to 4 millimeters, with implant survival rates reaching 95 to 100 percent over medium‑term follow‑ups. Direct lateral sinus lifts without grafts have also shown meaningful bone formation ranging from about 2.5 to over 6 millimeters, again with high implant success.
Comparative data indicate that although grafted sinus lifts may achieve slightly greater bone height increases, osseotransportation techniques still provide clinically sufficient bone for implant support in well‑selected cases. Importantly, osseotransportation procedures eliminate risks associated with graft materials, such as infection, graft resorption, and donor‑site morbidity, and reduce surgical complexity and cost.
From a biomechanical perspective, the newly formed bone in osseotransportation cases demonstrates adequate quality and density to support implant osseointegration. Histologic evaluations confirm the maturation of bone over time, with incorporation of lamellar bone and remodeling consistent with typical healing trajectories.
Indications, Advantages, and Limitations in Practice
Indications of Osseotransportation
Osseotransportation is most appropriate for patients with:
Moderate residual bone height (typically 4–6 mm)
Adequate bone quality in the basal bone
No active sinus pathology
Good overall systemic health
Advantages of Osseotransportation
Reduced surgical morbidity compared with graft harvesting
Elimination of graft‑related complications
Lower treatment cost
Shortened overall treatment time in selected protocols
Utilization of the patient’s own regenerative potential
Limitations of Osseotransportation
Technique sensitivity demands high surgical expertise
Limited vertical bone gain compared with some grafted protocols
Not suitable for severely atrophic maxillae with minimal residual bone
Dependence on maintaining an intact and stable sinus membrane
Careful patient selection, thorough preoperative imaging, and mastery of surgical subtleties are essential to maximize the benefits of this concept.
Practical Considerations for Osseotransportation
For clinicians implementing osseotransportation in sinus lifting, practice standards should emphasize:
Preoperative Assessment
Use cone‑beam computed tomography to evaluate sinus anatomy, residual bone height, and membrane thickness.Atraumatic Technique
Protect the Schneiderian membrane during elevation. Even small perforations can compromise the regenerative environment.Space Maintenance
Whether using implant apices, tenting screws, or specialized devices, a consistent space under the lifted membrane is fundamental to bone formation.Primary Stability
Ensure that implants achieve sufficient primary stability for predictable osseointegration in graftless environments.Postoperative Care
Follow conservative postoperative protocols to prevent sinus pressure changes that may disrupt the forming clot.
By incorporating these considerations, dental professionals can responsibly expand their sinus augmentation repertoire to include biologically driven osseotransportation techniques.
References (APA Style)
Bioresorption and bone formation dynamics following sinus membrane elevation.
Clinical outcomes of osteotome sinus floor elevation without grafting.
Direct lateral sinus lifts and graftless bone formation.
Comparative histologic studies of grafted vs graftless sinus augmentation.
Crestal hydraulic and balloon sinus elevation approaches.
Osseodensification in sinus lift procedures.
Frequently Asked Questions (FAQ)
1. What is the osseotransportation concept in sinus lifting?
The osseotransportation concept refers to creating and maintaining a space beneath the elevated sinus membrane to stimulate the body’s natural bone‑forming processes, minimizing or eliminating the need for bone graft materials.
2. How does bone form without graft material in sinus lifts?
Bone formation occurs when the elevated Schneiderian membrane and stabilized space allow a blood clot to form, serving as a scaffold that attracts osteogenic cells from adjacent bone and the membrane itself, leading to new bone deposition.
3. Is this approach suitable for all sinus augmentation cases?
No. Osseotransportation is most successful in patients with moderate residual bone height and no severe sinus pathology. Cases with extremely low bone height may still require traditional grafting for extensive augmentation.
4. How much bone gain can be expected with this technique?
Vertical bone gain varies by technique and individual healing but typically ranges from 2 to over 6 millimeters in reported clinical series.
5. Are implant outcomes similar to grafted sinus lifts?
Yes. Studies show that implant survival rates with osseotransportation techniques are comparable to traditional grafted sinus lifts, often exceeding 95% in well‑selected cases.
6. What are the main advantages of osseotransportation?
The key advantages include reduced morbidity, fewer graft‑related complications, lower cost, and a biologically natural pathway to bone regeneration with shorter overall treatment time in select protocols.
Recent Articles




























The posterior maxilla presents a unique challenge in implant dentistry due to reduced bone height, compromised bone quality, and the proximity of the maxillary sinus. For decades, clinicians have used bone graft materials to augment this area before or during implant placement. However, evolving scientific evidence has introduced an alternative biologically driven strategy: the osseotransportation concept in sinus lifting. This approach emphasizes the body’s innate capacity for bone regeneration by creating and maintaining space beneath the elevated Schneiderian membrane without relying on large volumes of graft material.
This article explores the biological basis, clinical application, outcomes, and practical considerations of osseotransportation in sinus lifting, providing dental professionals with a comprehensive understanding of this evolving technique.
Understanding Osseotransportation in Sinus Lifting
The osseotransportation concept refers to the coordinated process by which bone is generated in the sinus cavity following elevation of the sinus membrane. Conventionally, sinus lifting has involved grafting with autogenous bone, allografts, xenografts, or synthetic substitutes to fill the space created between the sinus floor and the Schneiderian membrane. In contrast, osseotransportation relies on the body’s biological mechanisms to form bone once space is created and stabilized.
The premise is straightforward: space creation is the precursor to bone regeneration. When the sinus membrane is elevated and the created space is maintained — whether by the implant itself, specialized devices, or careful surgical manipulation — a stable blood clot forms. This blood clot, in combination with osteoprogenitor cells and growth factors from the surrounding bone and the membrane, becomes the scaffold for new bone formation. The osseotransportation concept aligns with key biological principles such as mechanotransduction and Wolff’s law, which underscore how functional loading and controlled space maintenance influence bone remodeling and growth.
Biological Basis Behind Osseotransportation and Bone Regeneration
At the core of the osseotransportation concept in sinus lifting is the biological activity of the Schneiderian membrane and the native bone. The Schneiderian membrane is not a passive lining; it contains cells capable of expressing osteogenic markers — indicating its potential to participate in bone formation. When elevated, this membrane contributes osteoprogenitor cells and biologically active signaling to the regenerative process.
Once the membrane is lifted, the resultant compartment is initially filled with a blood clot. This clot serves as a natural provisional matrix that supports the migration of mesenchymal stem cells and vascular ingrowth. The adjacent alveolar bone and lateral sinus walls provide sources of osteogenic cells that populate the space. Over time, these cells differentiate and deposit bone matrix, gradually transforming the space into mineralized bone.
This biological foundation shifts the paradigm from “filling” with bone substitutes to “facilitating” bone growth by maintaining a stable space under the membrane. It underscores why osseotransportation is increasingly embraced for cases where residual bone height is moderate and predictable bone gain is feasible.
Clinical Techniques and Protocols for Osseotransportation in Sinus Lifting
Several surgical techniques leverage the osseotransportation concept, and each aims to maintain the elevated sinus membrane and encourage native bone formation:
1- Indirect Sinus Lift (Osteotome Technique)
The indirect sinus lift, commonly performed using the osteotome technique, is a minimally invasive approach that allows elevation of the sinus floor through the crestal aspect of the alveolar ridge. Using specially designed osteotomes, the clinician carefully fractures and displaces the sinus floor upward, creating a space between the residual bone and the Schneiderian membrane. The space is naturally filled with a blood clot, which acts as a scaffold for bone regeneration. In many cases, the dental implant is placed simultaneously, with its apex helping to maintain the elevated space. This technique is particularly effective for patients with moderate residual bone height and offers reduced surgical morbidity compared to lateral approaches, while leveraging the body’s innate regenerative capacity for predictable bone formation.
2- Direct Lateral Window Approach Without Grafts
The direct lateral window sinus lift is indicated in cases with more pronounced bone deficiency, where the residual alveolar height may not be sufficient for an indirect approach. A small lateral window is created in the lateral wall of the maxillary sinus, allowing direct access to elevate the Schneiderian membrane carefully. Instead of introducing bone graft material, the elevated space relies on the stability of the membrane and the formation of a blood clot to induce new bone growth. This technique maximizes the regenerative potential of the sinus environment, reduces complications associated with graft materials, and allows simultaneous or delayed implant placement depending on primary stability and surgical considerations. Proper membrane handling and space maintenance are essential to achieve successful outcomes with this graftless approach.
3- Hydraulic and Balloon Elevation Techniques
Hydraulic and balloon sinus elevation techniques are modern alternatives to traditional sinus lifts, emphasizing atraumatic and controlled elevation of the Schneiderian membrane. Using either carefully controlled hydraulic pressure or small inflatable balloon devices, the sinus membrane is gently lifted to create the desired vertical space. Once elevated, the space is maintained by the implant itself or specialized tenting devices to support bone formation. These techniques reduce the risk of membrane perforation and patient morbidity, while promoting natural bone regeneration without the need for graft materials. Hydraulic and balloon methods are particularly beneficial in cases where precision and minimally invasive approaches are desired, offering predictable vertical bone gain and high implant success rates.
4- Osseodensification‑Assisted Sinus Lift
Osseodensification-assisted sinus lifts utilize specially designed drills that compact, rather than remove, bone during preparation of the osteotomy site. This compaction increases bone density and simultaneously elevates the sinus membrane, creating a stable space for bone regeneration. By enhancing the primary stability of the implant and maintaining the sinus elevation, this technique leverages both mechanical and biological principles to support bone formation without graft materials. Osseodensification is particularly advantageous in patients with low to moderate residual bone height, where conventional drilling might compromise bone integrity. The technique also improves implant stability, reduces micromovement, and creates an environment conducive to predictable osseointegration in graftless sinus augmentation procedures.
Across all techniques, the clinician’s skill in membrane management, atraumatic elevation, and space maintenance is critical. Avoiding membrane tears and ensuring primary implant stability are prerequisites for predictable outcomes.
5- Sinus Lift Implant (SinusFuse): Achieving More With Less
SinusFuse is an advanced dental implant engineered to function simultaneously as a sinus lift instrument and a definitive implant, redefining efficiency in posterior maxillary rehabilitation. Its patented apical blades are specifically designed to gently up-fracture the sinus floor while minimizing the risk of Schneiderian membrane perforation. A unique reverse helical side-cut geometry allows autogenous bone to be shaved during insertion and immediately transported internally toward the elevated sinus space. These bone particles are preserved within a concave, dish-shaped apical reservoir, enabling controlled osseotransportation without external exposure or contamination. By harvesting, transporting, and stabilizing the patient’s own bone in a single step, SinusFuse achieves predictable sinus elevation and bone regeneration with reduced surgical complexity and biological compromise.
Interested in knowing more about Sinusfuse? Read the article :
Clinical Outcomes, Bone Gain, and Implant Survival
A substantial body of clinical evidence supports the effectiveness of osseotransportation in sinus lifting. Multiple studies demonstrate that adequate vertical bone gain and high implant survival rates can be achieved without the use of bone grafts.
For indirect sinus lift procedures performed without graft material, studies have reported average vertical bone gains of approximately 2 to 4 millimeters, with implant survival rates reaching 95 to 100 percent over medium‑term follow‑ups. Direct lateral sinus lifts without grafts have also shown meaningful bone formation ranging from about 2.5 to over 6 millimeters, again with high implant success.
Comparative data indicate that although grafted sinus lifts may achieve slightly greater bone height increases, osseotransportation techniques still provide clinically sufficient bone for implant support in well‑selected cases. Importantly, osseotransportation procedures eliminate risks associated with graft materials, such as infection, graft resorption, and donor‑site morbidity, and reduce surgical complexity and cost.
From a biomechanical perspective, the newly formed bone in osseotransportation cases demonstrates adequate quality and density to support implant osseointegration. Histologic evaluations confirm the maturation of bone over time, with incorporation of lamellar bone and remodeling consistent with typical healing trajectories.
Indications, Advantages, and Limitations in Practice
Indications of Osseotransportation
Osseotransportation is most appropriate for patients with:
Moderate residual bone height (typically 4–6 mm)
Adequate bone quality in the basal bone
No active sinus pathology
Good overall systemic health
Advantages of Osseotransportation
Reduced surgical morbidity compared with graft harvesting
Elimination of graft‑related complications
Lower treatment cost
Shortened overall treatment time in selected protocols
Utilization of the patient’s own regenerative potential
Limitations of Osseotransportation
Technique sensitivity demands high surgical expertise
Limited vertical bone gain compared with some grafted protocols
Not suitable for severely atrophic maxillae with minimal residual bone
Dependence on maintaining an intact and stable sinus membrane
Careful patient selection, thorough preoperative imaging, and mastery of surgical subtleties are essential to maximize the benefits of this concept.
Practical Considerations for Osseotransportation
For clinicians implementing osseotransportation in sinus lifting, practice standards should emphasize:
Preoperative Assessment
Use cone‑beam computed tomography to evaluate sinus anatomy, residual bone height, and membrane thickness.Atraumatic Technique
Protect the Schneiderian membrane during elevation. Even small perforations can compromise the regenerative environment.Space Maintenance
Whether using implant apices, tenting screws, or specialized devices, a consistent space under the lifted membrane is fundamental to bone formation.Primary Stability
Ensure that implants achieve sufficient primary stability for predictable osseointegration in graftless environments.Postoperative Care
Follow conservative postoperative protocols to prevent sinus pressure changes that may disrupt the forming clot.
By incorporating these considerations, dental professionals can responsibly expand their sinus augmentation repertoire to include biologically driven osseotransportation techniques.
References (APA Style)
Bioresorption and bone formation dynamics following sinus membrane elevation.
Clinical outcomes of osteotome sinus floor elevation without grafting.
Direct lateral sinus lifts and graftless bone formation.
Comparative histologic studies of grafted vs graftless sinus augmentation.
Crestal hydraulic and balloon sinus elevation approaches.
Osseodensification in sinus lift procedures.
Frequently Asked Questions (FAQ)
1. What is the osseotransportation concept in sinus lifting?
The osseotransportation concept refers to creating and maintaining a space beneath the elevated sinus membrane to stimulate the body’s natural bone‑forming processes, minimizing or eliminating the need for bone graft materials.
2. How does bone form without graft material in sinus lifts?
Bone formation occurs when the elevated Schneiderian membrane and stabilized space allow a blood clot to form, serving as a scaffold that attracts osteogenic cells from adjacent bone and the membrane itself, leading to new bone deposition.
3. Is this approach suitable for all sinus augmentation cases?
No. Osseotransportation is most successful in patients with moderate residual bone height and no severe sinus pathology. Cases with extremely low bone height may still require traditional grafting for extensive augmentation.
4. How much bone gain can be expected with this technique?
Vertical bone gain varies by technique and individual healing but typically ranges from 2 to over 6 millimeters in reported clinical series.
5. Are implant outcomes similar to grafted sinus lifts?
Yes. Studies show that implant survival rates with osseotransportation techniques are comparable to traditional grafted sinus lifts, often exceeding 95% in well‑selected cases.
6. What are the main advantages of osseotransportation?
The key advantages include reduced morbidity, fewer graft‑related complications, lower cost, and a biologically natural pathway to bone regeneration with shorter overall treatment time in select protocols.
Recent Articles

Peri-Implantitis Treatment & Prevention Methods
Peri-Implantitis Treatment & Prevention Methods Peri-implantitis remains one of the most significant biological complications affecting dental implants, posing a serious threat to long-term implant [...]
Latest Sinus Lifting Techniques in Modern Implant Dentistry
Latest Sinus Lifting Techniques in Modern Implant Dentistry A Comprehensive Clinical Review Introduction to Sinus Lifting in Implantology Sinus lifting, or maxillary sinus floor [...]

Biomechanics of the Triple Abutment & BOPiT Concept
Dental Biomechanics · Implant Science · Clinical Evidence Biomechanics of the Triple Abutment & BOPiT Concept How a saddle-shaped mathematical surface is rewriting the rules of load distribution [...]

The Woman Who Proved One Implant Could Hold Three Crowns
The Woman Who Proved One Implant Could Hold Three Crowns While the dental establishment looked away, Dr. Luciana Colepícolo spent 12 years building the [...]
ENPP1, The Molecular Brake That Limits Tissue Healing
ENPP1, The Molecular Brake That Limits Tissue Healing Introduction: A New Biological Barrier to Dental Regeneration Meet ENPP1—a protein most dentists have never heard [...]
The Rise of Self‑Healing Dental Biomaterials
The Rise of Self‑Healing Dental Biomaterials Introduction In modern restorative dentistry, durability and longevity of materials remain among the greatest clinical challenges. Traditional dental [...]








{kind=link}
{kind=link}
{kind=link}