

Peri-Implantitis Treatment & Prevention Methods
Peri-implantitis remains one of the most significant biological complications affecting dental implants, posing a serious threat to long-term implant success. As implant dentistry continues to evolve, clinicians must adopt a proactive and evidence-based approach to both the prevention and management of peri-implant diseases. This article provides a comprehensive overview of peri-implantitis, including its etiology, risk factors, diagnostic criteria, and the latest treatment and prevention strategies.
Understanding Peri-Implantitis
Peri-implantitis is defined as a pathological condition characterized by inflammation of peri-implant tissues accompanied by progressive bone loss. It typically develops from untreated peri-implant mucositis, which is a reversible inflammatory condition limited to the soft tissues surrounding an implant.
Clinically, peri-implantitis presents with:
- Bleeding on probing (BOP)
- Suppuration
- Increased probing depth
- Radiographic bone loss beyond initial remodeling
The disease is primarily biofilm-induced but is strongly influenced by systemic, local, and iatrogenic factors.
—
Etiology and Risk Factors
1. Bacterial Biofilm
The primary etiological factor is the accumulation of pathogenic biofilm on implant surfaces. The microbial profile is similar to periodontitis, dominated by anaerobic Gram-negative bacteria.
2. History of Periodontitis
Patients with a prior history of periodontal disease exhibit a significantly higher risk of developing peri-implantitis due to a predisposed inflammatory response.
3. Poor Oral Hygiene
Inadequate plaque control remains a major contributor, particularly in patients lacking proper maintenance protocols.
4. Smoking
Smoking impairs immune response and vascularization, increasing susceptibility to peri-implant tissue breakdown.
5. Prosthetic Design Factors
Overcontoured restorations, improper emergence profiles, and difficult-to-clean prostheses contribute to plaque accumulation.
6. Surgical and Positioning Errors
Incorrect implant placement, particularly too buccal or too deep, can compromise bone stability and soft tissue health.
—
Diagnosis of Peri-Implantitis
Accurate diagnosis is essential for timely intervention. Clinicians should rely on a combination of clinical and radiographic assessments:
- Baseline and follow-up probing depths
- Bleeding and suppuration on probing
- Standardized periapical radiographs
- Comparison with initial post-placement bone levels
Early detection significantly improves treatment outcomes.
—
Non-Surgical Treatment Methods
Non-surgical therapy is typically the first line of intervention, especially in early to moderate cases.
1. Mechanical Debridement
Mechanical removal of biofilm and calculus is performed using:
- Carbon fiber or titanium curettes
- Ultrasonic devices with implant-safe tips
This step is fundamental but often insufficient alone in advanced cases.
2. Antiseptic Therapy
Chlorhexidine (0.12%–0.2%) is commonly used as an adjunct to reduce microbial load.
3. Local Antibiotics
Locally delivered antimicrobials such as minocycline or doxycycline can enhance treatment outcomes by targeting residual bacteria.
4. Laser Therapy
Laser-assisted decontamination (e.g., diode or Er:YAG lasers) can improve bacterial reduction and promote tissue healing.
Surgical Treatment Methods
Advanced peri-implantitis cases often require surgical intervention to access and detoxify the implant surface and regenerate lost bone.
1. Open Flap Debridement
This approach allows direct visualization and thorough decontamination of implant surfaces.
2. Implant Surface Decontamination
Various methods are used, including:
- Air-abrasive systems (glycine powder)
- Chemical agents (hydrogen peroxide, EDTA)
- Laser decontamination
3. Resective Surgery
In cases with non-contained defects, resective therapy aims to reduce pocket depth and facilitate maintenance.
4. Regenerative Surgery
For contained defects, bone grafting combined with membranes can help restore lost bone. Materials include:
- Xenografts
- Allografts
- Synthetic bone substitutes
5. Implantoplasty
This involves smoothing exposed implant threads to reduce plaque retention and improve tissue adaptation.
—
Prevention of Peri-Implantitis
Prevention remains the most predictable strategy for managing peri-implant diseases. A structured protocol should be implemented at multiple levels:
1. Proper Case Selection
Careful evaluation of systemic health, smoking status, and periodontal history is critical before implant placement.
2. Prosthetically Driven Planning
Accurate implant positioning ensures optimal load distribution and facilitates hygiene access.
3. Surgical Precision
Minimizing trauma and ensuring adequate bone volume reduces the risk of future complications.
4. Maintenance Protocols
Regular follow-up visits (every 3–6 months) are essential for early detection and intervention.
5. Patient Education
Patients must be trained in effective oral hygiene practices, including:
- Use of interdental brushes
- Water flossers
- Implant-specific cleaning tools
6. Prosthetic Design Optimization
Restorations should be designed to allow easy cleaning, avoiding overcontouring and deep margins.
—
Emerging Technologies and Future Directions
Recent advancements are enhancing both diagnosis and treatment outcomes:
- Digital Implant Planning: Improves implant positioning and reduces biomechanical complications.
- Guided Surgery: Enhances surgical accuracy and minimizes errors.
- Biologics: Growth factors and PRF are being explored for regenerative therapy.
- Surface Modifications: New implant surfaces aim to reduce bacterial adhesion.
These innovations are expected to significantly reduce the incidence of peri-implantitis in the future.
—
Conclusion
Peri-implantitis is a complex and multifactorial condition that requires a comprehensive and multidisciplinary approach. While various treatment modalities exist, prevention remains the cornerstone of long-term implant success. Clinicians must integrate proper planning, precise surgical execution, and structured maintenance protocols to minimize risks and ensure optimal outcomes.
—
Frequently Asked Questions (FAQ)
1. What is the difference between peri-implant mucositis and peri-implantitis?
Peri-implant mucositis is a reversible inflammation limited to soft tissues, while peri-implantitis involves bone loss and is more severe.
2. Can peri-implantitis be completely cured?
It can be controlled and stabilized, especially when detected early, but complete regeneration is not always predictable.
3. How common is peri-implantitis?
Studies suggest it affects approximately 10–20% of implant patients over time.
4. Is surgery always required?
No, early cases can often be managed non-surgically. Surgery is indicated in advanced stages.
5. How can patients prevent peri-implantitis?
By maintaining excellent oral hygiene, attending regular check-ups, and following professional maintenance programs.
6. Does implant surface type affect peri-implantitis risk?
Yes, rough surfaces may retain more biofilm, but they also improve osseointegration. Balance is key.
—
References
- Berglundh T, Armitage G, Araujo MG, et al. Peri-implant diseases and conditions: Consensus report. Journal of Clinical Periodontology.
- Schwarz F, Derks J, Monje A, Wang HL. Peri-implantitis. Journal of Periodontology.
- Lindhe J, Meyle J. Peri-implant diseases: Consensus Report of the Sixth European Workshop on Periodontology.
- Heitz-Mayfield LJ. Peri-implant diseases: diagnosis and risk indicators. Journal of Clinical Periodontology.
- Renvert S, Polyzois I. Treatment of pathologic peri-implant pockets. Periodontology 2000.
- Esposito M, Grusovin MG, Worthington HV. Treatment of peri-implantitis: systematic review. European Journal of Oral Implantology.
- Figuero E, Graziani F, Sanz I, Herrera D, Sanz M. Management of peri-implant mucositis and peri-implantitis. Periodontology 2000.
Recent Articles





































Peri-implantitis remains one of the most significant biological complications affecting dental implants, posing a serious threat to long-term implant success. As implant dentistry continues to evolve, clinicians must adopt a proactive and evidence-based approach to both the prevention and management of peri-implant diseases. This article provides a comprehensive overview of peri-implantitis, including its etiology, risk factors, diagnostic criteria, and the latest treatment and prevention strategies.
Understanding Peri-Implantitis
Peri-implantitis is defined as a pathological condition characterized by inflammation of peri-implant tissues accompanied by progressive bone loss. It typically develops from untreated peri-implant mucositis, which is a reversible inflammatory condition limited to the soft tissues surrounding an implant.
Clinically, peri-implantitis presents with:
- Bleeding on probing (BOP)
- Suppuration
- Increased probing depth
- Radiographic bone loss beyond initial remodeling
The disease is primarily biofilm-induced but is strongly influenced by systemic, local, and iatrogenic factors.
—
Etiology and Risk Factors
1. Bacterial Biofilm
The primary etiological factor is the accumulation of pathogenic biofilm on implant surfaces. The microbial profile is similar to periodontitis, dominated by anaerobic Gram-negative bacteria.
2. History of Periodontitis
Patients with a prior history of periodontal disease exhibit a significantly higher risk of developing peri-implantitis due to a predisposed inflammatory response.
3. Poor Oral Hygiene
Inadequate plaque control remains a major contributor, particularly in patients lacking proper maintenance protocols.
4. Smoking
Smoking impairs immune response and vascularization, increasing susceptibility to peri-implant tissue breakdown.
5. Prosthetic Design Factors
Overcontoured restorations, improper emergence profiles, and difficult-to-clean prostheses contribute to plaque accumulation.
6. Surgical and Positioning Errors
Incorrect implant placement, particularly too buccal or too deep, can compromise bone stability and soft tissue health.
—
Diagnosis of Peri-Implantitis
Accurate diagnosis is essential for timely intervention. Clinicians should rely on a combination of clinical and radiographic assessments:
- Baseline and follow-up probing depths
- Bleeding and suppuration on probing
- Standardized periapical radiographs
- Comparison with initial post-placement bone levels
Early detection significantly improves treatment outcomes.
—
Non-Surgical Treatment Methods
Non-surgical therapy is typically the first line of intervention, especially in early to moderate cases.
1. Mechanical Debridement
Mechanical removal of biofilm and calculus is performed using:
- Carbon fiber or titanium curettes
- Ultrasonic devices with implant-safe tips
This step is fundamental but often insufficient alone in advanced cases.
2. Antiseptic Therapy
Chlorhexidine (0.12%–0.2%) is commonly used as an adjunct to reduce microbial load.
3. Local Antibiotics
Locally delivered antimicrobials such as minocycline or doxycycline can enhance treatment outcomes by targeting residual bacteria.
4. Laser Therapy
Laser-assisted decontamination (e.g., diode or Er:YAG lasers) can improve bacterial reduction and promote tissue healing.
Surgical Treatment Methods
Advanced peri-implantitis cases often require surgical intervention to access and detoxify the implant surface and regenerate lost bone.
1. Open Flap Debridement
This approach allows direct visualization and thorough decontamination of implant surfaces.
2. Implant Surface Decontamination
Various methods are used, including:
- Air-abrasive systems (glycine powder)
- Chemical agents (hydrogen peroxide, EDTA)
- Laser decontamination
3. Resective Surgery
In cases with non-contained defects, resective therapy aims to reduce pocket depth and facilitate maintenance.
4. Regenerative Surgery
For contained defects, bone grafting combined with membranes can help restore lost bone. Materials include:
- Xenografts
- Allografts
- Synthetic bone substitutes
5. Implantoplasty
This involves smoothing exposed implant threads to reduce plaque retention and improve tissue adaptation.
—
Prevention of Peri-Implantitis
Prevention remains the most predictable strategy for managing peri-implant diseases. A structured protocol should be implemented at multiple levels:
1. Proper Case Selection
Careful evaluation of systemic health, smoking status, and periodontal history is critical before implant placement.
2. Prosthetically Driven Planning
Accurate implant positioning ensures optimal load distribution and facilitates hygiene access.
3. Surgical Precision
Minimizing trauma and ensuring adequate bone volume reduces the risk of future complications.
4. Maintenance Protocols
Regular follow-up visits (every 3–6 months) are essential for early detection and intervention.
5. Patient Education
Patients must be trained in effective oral hygiene practices, including:
- Use of interdental brushes
- Water flossers
- Implant-specific cleaning tools
6. Prosthetic Design Optimization
Restorations should be designed to allow easy cleaning, avoiding overcontouring and deep margins.
—
Emerging Technologies and Future Directions
Recent advancements are enhancing both diagnosis and treatment outcomes:
- Digital Implant Planning: Improves implant positioning and reduces biomechanical complications.
- Guided Surgery: Enhances surgical accuracy and minimizes errors.
- Biologics: Growth factors and PRF are being explored for regenerative therapy.
- Surface Modifications: New implant surfaces aim to reduce bacterial adhesion.
These innovations are expected to significantly reduce the incidence of peri-implantitis in the future.
—
Conclusion
Peri-implantitis is a complex and multifactorial condition that requires a comprehensive and multidisciplinary approach. While various treatment modalities exist, prevention remains the cornerstone of long-term implant success. Clinicians must integrate proper planning, precise surgical execution, and structured maintenance protocols to minimize risks and ensure optimal outcomes.
—
Frequently Asked Questions (FAQ)
1. What is the difference between peri-implant mucositis and peri-implantitis?
Peri-implant mucositis is a reversible inflammation limited to soft tissues, while peri-implantitis involves bone loss and is more severe.
2. Can peri-implantitis be completely cured?
It can be controlled and stabilized, especially when detected early, but complete regeneration is not always predictable.
3. How common is peri-implantitis?
Studies suggest it affects approximately 10–20% of implant patients over time.
4. Is surgery always required?
No, early cases can often be managed non-surgically. Surgery is indicated in advanced stages.
5. How can patients prevent peri-implantitis?
By maintaining excellent oral hygiene, attending regular check-ups, and following professional maintenance programs.
6. Does implant surface type affect peri-implantitis risk?
Yes, rough surfaces may retain more biofilm, but they also improve osseointegration. Balance is key.
—
References
- Berglundh T, Armitage G, Araujo MG, et al. Peri-implant diseases and conditions: Consensus report. Journal of Clinical Periodontology.
- Schwarz F, Derks J, Monje A, Wang HL. Peri-implantitis. Journal of Periodontology.
- Lindhe J, Meyle J. Peri-implant diseases: Consensus Report of the Sixth European Workshop on Periodontology.
- Heitz-Mayfield LJ. Peri-implant diseases: diagnosis and risk indicators. Journal of Clinical Periodontology.
- Renvert S, Polyzois I. Treatment of pathologic peri-implant pockets. Periodontology 2000.
- Esposito M, Grusovin MG, Worthington HV. Treatment of peri-implantitis: systematic review. European Journal of Oral Implantology.
- Figuero E, Graziani F, Sanz I, Herrera D, Sanz M. Management of peri-implant mucositis and peri-implantitis. Periodontology 2000.
Recent Articles
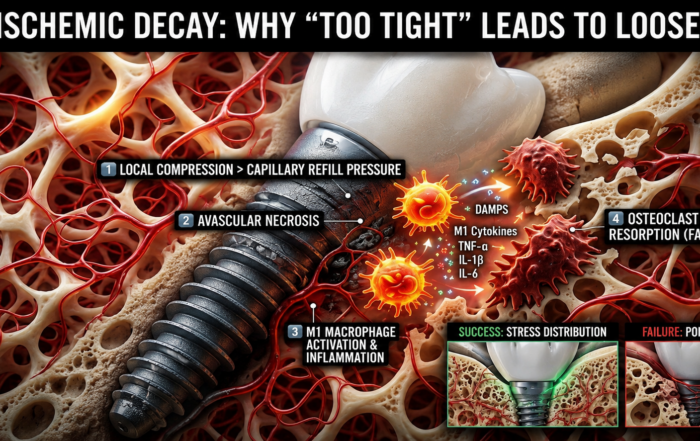
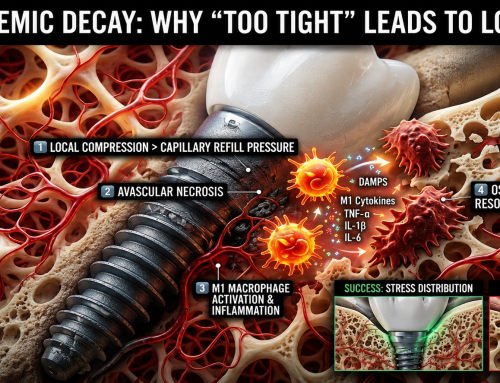
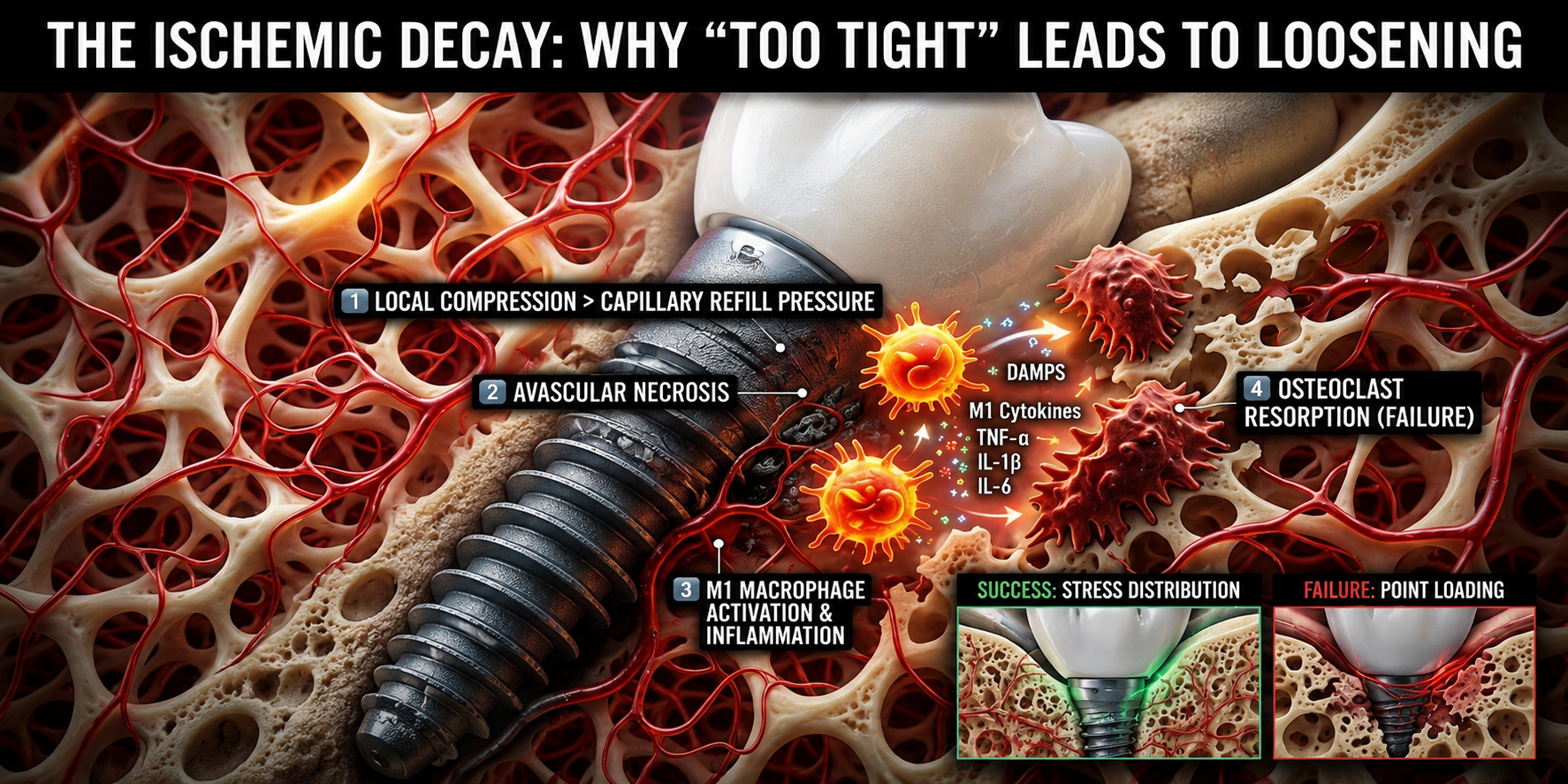
When “Perfectly Tight” Dental Implants Fail
When “Perfectly Tight” Dental Implants Fail The Hidden Role of Ischemic Bone Resorption and Osteoimmune Dysfunction In modern dental implantology, achieving high primary [...]

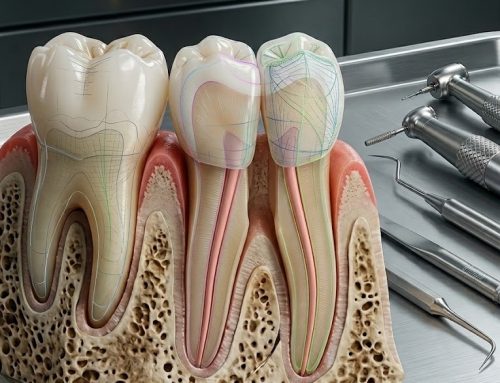
The Bicuspidization Protocol: Engineering Meets Survival
The Bicuspidization Protocol: Engineering Meets Survival Modern restorative dentistry is no longer limited to extraction and replacement. In the era of conservative and biologically [...]
Pulsed Electromagnetic Field (PEMF) Use in Implant Dentistry
Pulsed Electromagnetic Field (PEMF) Use in Implant Dentistry Abstract and Historical Background Pulsed Electromagnetic Field (PEMF) therapy refers to the application of low-frequency electromagnetic [...]
Laser Therapy in the Management of Peri-Implantitis
Laser Therapy in the Management of Peri-Implantitis Laser technology has become an increasingly valuable adjunct in the treatment of peri-implant diseases, particularly peri-implantitis. Its [...]
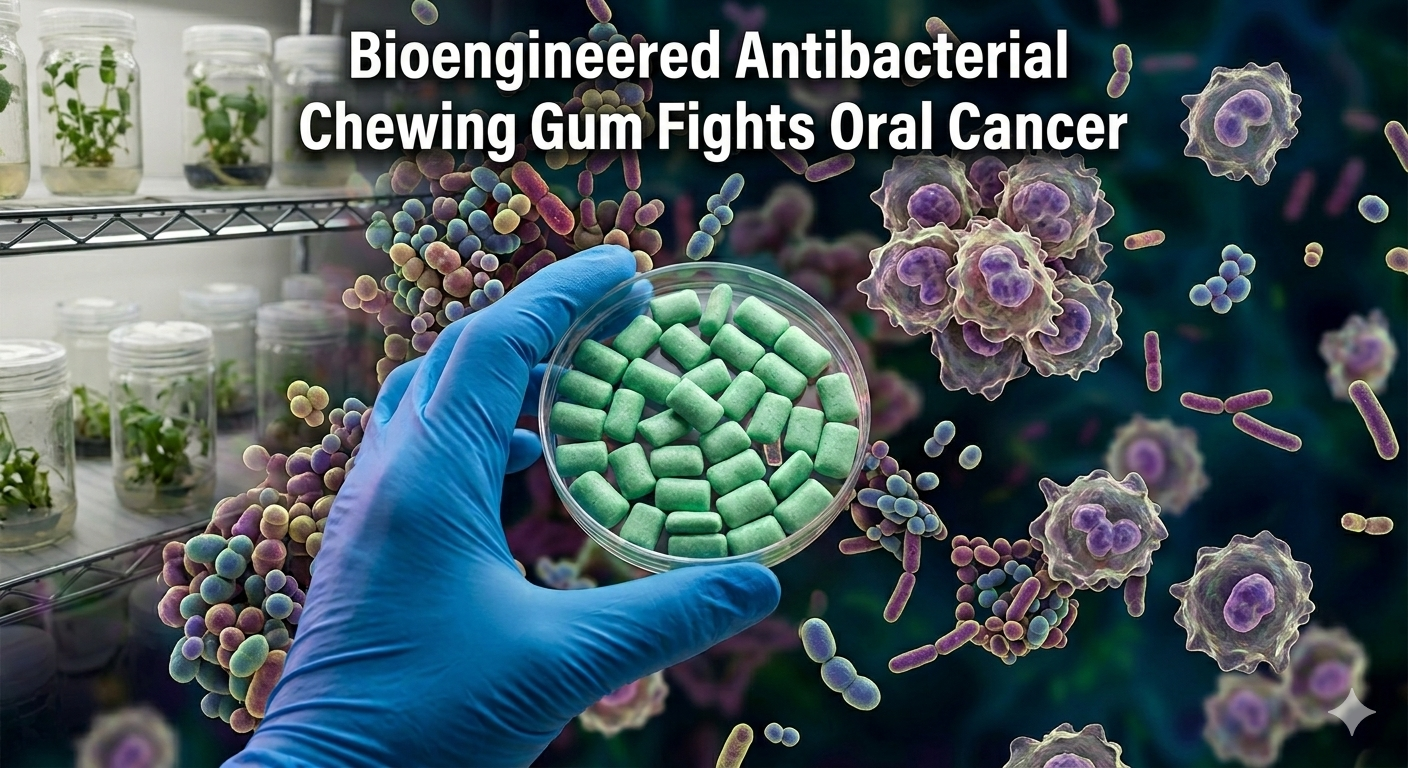
Magnetically Guided Dental Nanobots (CalBots) Are Real
Magnetically Guided Dental Nanobots (CalBots) Are Real The concept of nanobots in dentistry has long been associated with futuristic speculation. However, recent peer-reviewed research [...]

Peri-Implantitis Treatment & Prevention Methods
Peri-Implantitis Treatment & Prevention Methods Peri-implantitis remains one of the most significant biological complications affecting dental implants, posing a serious threat to long-term implant [...]
{kind=link}
{kind=link}
{kind=link}