

The Woman Who Proved One Implant Could Hold Three Crowns
While the dental establishment looked away, Dr. Luciana Colepícolo spent 12 years building the evidence. The results are impossible to ignore.
A Concept Born in a Brazilian Clinic, And Dismissed Without a Reading
In implant dentistry, paradigms die hard. The field has operated for decades on a straightforward premise: one implant, one crown. To suggest otherwise was to invite skepticism at best, and mockery at worst. Dr. Luciana Silva Colepícolo, a Brazilian dentist and researcher at the Federal University of Minas Gerais, learned this firsthand.
Her idea was deceptively elegant: what if the geometry of a dental abutment could be redesigned, not incrementally, but fundamentally, to redistribute masticatory forces so efficiently that a single osseointegrated implant could support two or even three crowns, without welding, without cantilevers, and without compromising the health of the surrounding bone?
Some in the field laughed. Some dismissed the concept without engaging with a single page of the clinical data. The kind of dismissal that has, throughout history, preceded nearly every meaningful advance in medicine.
They didn’t read the 12 years of follow-up data. They didn’t look at the radiographs showing bone stability that rivals conventional single-crown implants. They didn’t engage with the biomechanical logic, rooted in mathematics, not opinion.
This article exists to correct that oversight.
“The manner in which occlusal loads are transferred to the bone-implant interface via superstructures is considered a crucial factor for the success of implant treatment — its mechanical properties interfere directly with the magnitude of occlusal forces.“
Colepícolo et al., Clinical Advances in Periodontics, 2024

What Exactly Is the Triple Abutment, and Why Does Its Geometry Matter?
To understand what Dr. Colepícolo invented, you first need to understand what was missing in the field. Every dental abutment on the market today shares the same fundamental design heritage: cylindrical. Whether the connection is an internal hexagon, external hexagon, or conical taper, the abutment’s prosthetic geometry remains rooted in a shape that concentrates stress, depends on parallelism between implants, and cannot function across multiple crowns without welds or bars that introduce their own distortion risks.
The Triple Abutment (TA) breaks all of this. Its geometry is derived not from convention, but from mathematics — specifically, from the hyperbolic paraboloid, a doubly-ruled saddle surface that opens downward along one axis and upward along another.

TA Triple Abutment Concept by Dr. Luciana
Why a Hyperbolic Paraboloid?
This shape, familiar to architects as one of the most efficient load-distributing structures in nature and engineering, provides maximum rigidity with reduced bending stress. In the context of an implant abutment, it means that masticatory forces are not channeled toward the implant-abutment connection (where bone loss classically originates) but instead dispersed vectorially across the entire structure before they even reach the critical zone.
The result: less stress at the implant platform, less stress at the screw, and a bone interface that sees loading it can tolerate and even benefit from — the very definition of mechanobiological optimization.

This is not a theoretical claim. It is the conclusion of a finite element analysis study published in January 2026, comparing the TA abutment with both ceramic (zirconia) and titanium implants under simulated axial and oblique occlusal loads. The bone stress differences between the two implant materials were less than 5% — clinically negligible — while both configurations demonstrated biomechanical performance well within safe limits.
BOPiT: A Framework That Rethinks How Implants Communicate with Living Bone
Dr. Colepícolo did not stop at redesigning a component. She articulated an entirely new conceptual framework — Biodynamically Optimized Peri-implant Tissue (BOPiT) — to explain why this geometry produces the clinical outcomes it does.
BOPiT integrates three bodies of scientific knowledge that had not previously been brought together in implant abutment design:
- Bone mechanotransduction — the biological process by which bone cells convert mechanical signals into biochemical responses that drive remodeling, adaptation, and health maintenance
- Biotensegrity — the principle that biological structures maintain integrity not through rigid compression but through a dynamic balance of tension and compression distributed across the entire system
- Mechanobiology — the study of how physical forces regulate cell behavior, tissue development, and homeostasis at the molecular level
What BOPiT proposes — and what 12 years of clinical data supports — is that the geometry of a prosthetic abutment is not merely a mechanical connector. It is an information channel. The shape of the abutment determines the quality, direction, and magnitude of mechanical signals delivered to peri-implant tissues. Get the geometry right, and those tissues respond by maintaining health. Get it wrong, and they respond with inflammation, resorption, and failure.

“The quadric surfaces of these new abutments allow an instantaneous vectorial distribution of the received masticatory loads… A primary biophysical dissipation of stresses occurs in the abutment before they reach the attachment site of the implant-abutment connections.”
Colepícolo et al., Clinical Advances in Periodontics, 2024
The Data Does Not Lie: 12 Years of Peri-implant Health
The case study published in Clinical Advances in Periodontics (2024) represents one of the most carefully documented consecutive case series in modern implant dentistry. Forty-three implants in 37 patients — non-diabetic, non-smokers, spanning both maxilla and mandible, predominantly in the posterior region — were followed for an average of 7.2 years, with the longest cases exceeding a decade.
These were not ideal cases selected to flatter the results. Many involved implants placed in the absence of perfect parallelism conditions that would typically necessitate complex surgical or prosthetic workarounds. The TA abutment was chosen precisely because it functions where traditional systems require compromises.

To put the marginal bone loss figure in context: the threshold conventionally cited as compatible with peri-implant health in prospective studies is approximately 0.1–0.2 mm annually. The TA cases averaged 0.022 mm per year — a figure that not only clears the threshold but suggests the hyperbolic paraboloid geometry may actively promote bone homeostasis rather than merely tolerating it.
The radiographic panels in the published paper are equally compelling. At final examination, images show no angular bone defects, no craters, and favorable cortical thickness and trabecular mineralization — characteristics more commonly associated with pristine natural teeth than with prosthetic implant sites approaching a decade of function.

Ceramic or Titanium? The TA Abutment Makes It a Clinical Choice, Not a Structural One
The most recent publication from Dr. Colepícolo’s team — a finite element analysis study from January 2026 — addresses a question increasingly important to contemporary implant practice: can the TA system be used with zirconia (ceramic) implants, which many patients now request for aesthetic and biocompatibility reasons?
The analysis simulated both axial loading (250 N, distributed across occlusal fossae) and oblique loading (100 N at 45°) on two models: a TA with a zirconia implant and metal-ceramic crowns, and a TA with a conventional titanium implant and metal-ceramic crowns. Both used a Morse-taper implant placed 2 mm below the cortical surface in a Type 3 bone block derived from CT data of a real dentate maxilla.

The Bottom Line from the FEA Study
The ceramic (zirconia) model showed 10–20% higher stress in prosthetic components compared to titanium — an expected consequence of zirconia’s higher elastic modulus (205 GPa vs. 105 GPa for titanium). However, stress and microstrain values in the surrounding bone differed by less than 5% between the two models. Both remained well within clinically acceptable limits, and neither model showed failure regions attributable to material differences.
The conclusion is both practical and liberating for clinicians: implant material selection in the TA system can be guided by aesthetic and biocompatibility priorities without compromising biomechanical outcomes. Patients who want ceramic implants for the look, the hypoallergenic profile, or the thermal comfort — they can have them, with the same structural confidence.
This matters because the clinical barriers to ceramic implants have historically included uncertainty about stress distribution. The TA’s hyperbolic paraboloid geometry, by distributing forces so efficiently, appears to neutralize the material-specific disadvantages of zirconia at the bone interface — the site that actually determines long-term success.
What the TA System Offers That Conventional Implantology Cannot
For clinicians evaluating whether to engage with this research, the advantages of the TA and DA (Double Abutment) system extend well beyond the biomechanical:
- Rehabilitation of 2–3 element edentulous spans with a single implant — reducing surgical sites, patient morbidity, cost, and healing time
- No welding required — the system is fully passive, eliminating distortion risks introduced by conventional bar or bridge fabrication steps
- Function in inclined implant situations — where traditional systems require parallelism, the TA’s geometry accommodates angulation without compromise
- Elimination of cantilever mechanics — replacing a prosthetic solution known for unfavorable force distribution with one that actively optimizes it
- Natural hygiene compatibility — the parabolic emergence profile of the TA allows conventional dental floss use due to its segmented tripod configuration, supporting patient compliance
- Reduced stress at the implant platform and screw — the primary failure zones in conventional implant-abutment systems are depressurized by the TA’s geometric force dissipation
- Compatible with both ceramic and titanium implants — as confirmed by the 2026 FEA study, without clinically meaningful difference in bone behavior
- Multiple international patents — protecting the design across Brazil, India, Europe, and the United States
It bears stating plainly: this is not a system that asks clinicians to trade outcomes for convenience. The marginal bone loss data across 12 years of follow-up is better than what many conventional single-crown implant studies report. The peri-implant tissue parameters at final examination reflect health, not compromise. And the biomechanical modeling confirms that the forces reaching the bone are within ranges that bone tissue handles well.
Dr. Luciana Colepícolo: The Scientist Behind the Breakthrough
Dr. Luciana Silva Colepícolo
The institutional response to genuinely novel ideas in medicine is rarely swift warmth. When a concept dismantles something that “has always been done this way” — in this case, the fundamental architecture of how implants support prostheses — the default reaction from established voices is often dismissal rather than dialogue.
This is not unique to Dr. Colepícolo’s experience. It is the pattern. And it is why the data matters so much. Not because it should be necessary to prove oneself through a decade of outcomes to earn a fair reading — but because when the data is this good, dismissal without engagement becomes increasingly difficult to sustain as a credible position.
The question for clinicians is not whether this research deserves attention. Twelve years of follow-up data, a peer-reviewed FEA comparison, registration at ClinicalTrials.gov, and ethics committee approval from the Federal University of Minas Gerais — that is not a fringe proposal. That is a body of evidence asking to be read seriously.
What the Research Acknowledges — and Why That Makes It More Credible
Good science is defined partly by its honesty about limitations. Dr. Colepícolo’s team is explicit about the constraints of the current evidence base. The case series, though extraordinary in its follow-up duration and the quality of outcomes documented, is a consecutive case study — not a randomized controlled trial. Radiographic standardization varied between baseline and follow-up due to the time span involved. The FEA study, while methodologically rigorous, uses simplified bone models that cannot fully capture physiological variables like temperature, oral fluids, bruxism, or dynamic masticatory muscle forces.
These are not weaknesses to hide. They are the honest boundaries of a research program at an early-to-intermediate stage — and notably, a research program that has already accumulated more longitudinal clinical data than many widely-adopted implant innovations had at equivalent stages of their development.
What the authors call for — and what the evidence justifies — is the next step: prospective randomized clinical trials comparing TA/DA systems with conventional abutments under controlled conditions. That is how a promising innovation becomes a validated standard of care. The groundwork has been laid. The 12-year data exists. The biomechanical modeling has been done. What is needed now is engagement — from researchers, from clinicians, and from institutions with the resources to run the trials.
To the Dentists Who Haven’t Read the Papers Yet: Here Is Your Invitation
The history of medicine is full of innovations that were laughed at before they were lived with. The idea that Helicobacter pylori causes ulcers. The germ theory of disease. The notion that surgeons should wash their hands. Every one of them met resistance. Every one of them eventually prevailed, not because authority finally approved, but because the evidence accumulated beyond the point where dismissal was intellectually defensible.
Dr. Luciana Colepícolo has not asked for faith. She has published data. She has submitted to peer review. She has registered her clinical study. She has had her biomechanical models independently evaluated. She has followed patients for twelve years and documented the results with radiographs that are published, available, and clear.
The two papers referenced throughout this article are not difficult to find. They are in the peer-reviewed literature. They have reference lists. They have methods sections that describe exactly what was done and exactly what was measured. They are the kind of papers that, once read, make it very hard to return to the posture of dismissal without consequence.
“The proposed TA expands rehabilitation options by enabling the use of a single implant to support multiple crowns — with bone stress values similar between ceramic and titanium models, remaining within acceptable limits.”
Colepícolo et al., International Journal of Medical & Interdisciplinary Research, 2026
Colepícolo et al., International Journal of Medical & Interdisciplinary Research, 2026
For your patients who cannot afford multiple implants but need multiple crowns. For your patients who want ceramic implants but worry about structural performance. For your cases with non-ideal implant angulation. For every situation where conventional implantology forces a compromise, this research deserves your attention.
Read the papers. Look at the radiographs. Engage with the biomechanics. That is all the research has ever asked.
Further Reading
Primary Research References
- Colepícolo LS, Martinez MAM, Cota LOM, Lima RPE, Costa FO. Biomechanical Evaluation of An Innovative Triple Abutment System in Ceramic Versus Titanium Implants: A Finite Element Analysis. International Journal of Medical & Interdisciplinary Research. 2026 Jan;3(1):89–92.
- Colepícolo LS, Martinez MAM, Rodrigues AA, Baeta LS, Costa FO. The innovative double or triple dental abutment-implant: Case study with a 3-to-12-year follow-up. Clinical Advances in Periodontics. 2024. doi: 10.1002/cap
Patents: Brazil BR112020009609A2 · India 517585 · Europe 17932138.5 · USA 11,701,206 B2 | Clinical trial registration: NCT06127576 | Ethics approval: Federal University of Minas Gerais, Approval No. 5895732
The Research Is Published. The Data Is Clear. The Next Step Is Yours.
Read the original papers, share them with your colleagues, and consider what this geometry could mean for your most challenging implant cases.
READY TO JOIN THE REVOLUTION?
Fill in the form by clicking the button below:
This article is a professional editorial summary prepared to support awareness of peer-reviewed research by Dr. Luciana Silva Colepícolo and colleagues at the Federal University of Minas Gerais, Brazil.
All clinical data, statistics, and quotations are drawn directly from the published peer-reviewed papers cited above. No findings have been extrapolated or embellished.
Recent Articles





































While the dental establishment looked away, Dr. Luciana Colepícolo spent 12 years building the evidence. The results are impossible to ignore.
A Concept Born in a Brazilian Clinic, And Dismissed Without a Reading
In implant dentistry, paradigms die hard. The field has operated for decades on a straightforward premise: one implant, one crown. To suggest otherwise was to invite skepticism at best, and mockery at worst. Dr. Luciana Silva Colepícolo, a Brazilian dentist and researcher at the Federal University of Minas Gerais, learned this firsthand.
Her idea was deceptively elegant: what if the geometry of a dental abutment could be redesigned, not incrementally, but fundamentally, to redistribute masticatory forces so efficiently that a single osseointegrated implant could support two or even three crowns, without welding, without cantilevers, and without compromising the health of the surrounding bone?
Some in the field laughed. Some dismissed the concept without engaging with a single page of the clinical data. The kind of dismissal that has, throughout history, preceded nearly every meaningful advance in medicine.
They didn’t read the 12 years of follow-up data. They didn’t look at the radiographs showing bone stability that rivals conventional single-crown implants. They didn’t engage with the biomechanical logic, rooted in mathematics, not opinion.
This article exists to correct that oversight.
“The manner in which occlusal loads are transferred to the bone-implant interface via superstructures is considered a crucial factor for the success of implant treatment — its mechanical properties interfere directly with the magnitude of occlusal forces.“
Colepícolo et al., Clinical Advances in Periodontics, 2024
What Exactly Is the Triple Abutment, and Why Does Its Geometry Matter?
To understand what Dr. Colepícolo invented, you first need to understand what was missing in the field. Every dental abutment on the market today shares the same fundamental design heritage: cylindrical. Whether the connection is an internal hexagon, external hexagon, or conical taper, the abutment’s prosthetic geometry remains rooted in a shape that concentrates stress, depends on parallelism between implants, and cannot function across multiple crowns without welds or bars that introduce their own distortion risks.
The Triple Abutment (TA) breaks all of this. Its geometry is derived not from convention, but from mathematics — specifically, from the hyperbolic paraboloid, a doubly-ruled saddle surface that opens downward along one axis and upward along another.
TA Triple Abutment Concept by Dr. Luciana
Why a Hyperbolic Paraboloid?
This shape, familiar to architects as one of the most efficient load-distributing structures in nature and engineering, provides maximum rigidity with reduced bending stress. In the context of an implant abutment, it means that masticatory forces are not channeled toward the implant-abutment connection (where bone loss classically originates) but instead dispersed vectorially across the entire structure before they even reach the critical zone.
The result: less stress at the implant platform, less stress at the screw, and a bone interface that sees loading it can tolerate and even benefit from — the very definition of mechanobiological optimization.
This is not a theoretical claim. It is the conclusion of a finite element analysis study published in January 2026, comparing the TA abutment with both ceramic (zirconia) and titanium implants under simulated axial and oblique occlusal loads. The bone stress differences between the two implant materials were less than 5% — clinically negligible — while both configurations demonstrated biomechanical performance well within safe limits.
BOPiT: A Framework That Rethinks How Implants Communicate with Living Bone
Dr. Colepícolo did not stop at redesigning a component. She articulated an entirely new conceptual framework — Biodynamically Optimized Peri-implant Tissue (BOPiT) — to explain why this geometry produces the clinical outcomes it does.
BOPiT integrates three bodies of scientific knowledge that had not previously been brought together in implant abutment design:
- Bone mechanotransduction — the biological process by which bone cells convert mechanical signals into biochemical responses that drive remodeling, adaptation, and health maintenance
- Biotensegrity — the principle that biological structures maintain integrity not through rigid compression but through a dynamic balance of tension and compression distributed across the entire system
- Mechanobiology — the study of how physical forces regulate cell behavior, tissue development, and homeostasis at the molecular level
What BOPiT proposes — and what 12 years of clinical data supports — is that the geometry of a prosthetic abutment is not merely a mechanical connector. It is an information channel. The shape of the abutment determines the quality, direction, and magnitude of mechanical signals delivered to peri-implant tissues. Get the geometry right, and those tissues respond by maintaining health. Get it wrong, and they respond with inflammation, resorption, and failure.
“The quadric surfaces of these new abutments allow an instantaneous vectorial distribution of the received masticatory loads… A primary biophysical dissipation of stresses occurs in the abutment before they reach the attachment site of the implant-abutment connections.”
Colepícolo et al., Clinical Advances in Periodontics, 2024
The Data Does Not Lie: 12 Years of Peri-implant Health
The case study published in Clinical Advances in Periodontics (2024) represents one of the most carefully documented consecutive case series in modern implant dentistry. Forty-three implants in 37 patients — non-diabetic, non-smokers, spanning both maxilla and mandible, predominantly in the posterior region — were followed for an average of 7.2 years, with the longest cases exceeding a decade.
These were not ideal cases selected to flatter the results. Many involved implants placed in the absence of perfect parallelism conditions that would typically necessitate complex surgical or prosthetic workarounds. The TA abutment was chosen precisely because it functions where traditional systems require compromises.
To put the marginal bone loss figure in context: the threshold conventionally cited as compatible with peri-implant health in prospective studies is approximately 0.1–0.2 mm annually. The TA cases averaged 0.022 mm per year — a figure that not only clears the threshold but suggests the hyperbolic paraboloid geometry may actively promote bone homeostasis rather than merely tolerating it.
The radiographic panels in the published paper are equally compelling. At final examination, images show no angular bone defects, no craters, and favorable cortical thickness and trabecular mineralization — characteristics more commonly associated with pristine natural teeth than with prosthetic implant sites approaching a decade of function.
Triple Abutment 7 year follow up by Dr. Luciana and her team
Ceramic or Titanium? The TA Abutment Makes It a Clinical Choice, Not a Structural One
The most recent publication from Dr. Colepícolo’s team — a finite element analysis study from January 2026 — addresses a question increasingly important to contemporary implant practice: can the TA system be used with zirconia (ceramic) implants, which many patients now request for aesthetic and biocompatibility reasons?
The analysis simulated both axial loading (250 N, distributed across occlusal fossae) and oblique loading (100 N at 45°) on two models: a TA with a zirconia implant and metal-ceramic crowns, and a TA with a conventional titanium implant and metal-ceramic crowns. Both used a Morse-taper implant placed 2 mm below the cortical surface in a Type 3 bone block derived from CT data of a real dentate maxilla.
The Bottom Line from the FEA Study
The ceramic (zirconia) model showed 10–20% higher stress in prosthetic components compared to titanium — an expected consequence of zirconia’s higher elastic modulus (205 GPa vs. 105 GPa for titanium). However, stress and microstrain values in the surrounding bone differed by less than 5% between the two models. Both remained well within clinically acceptable limits, and neither model showed failure regions attributable to material differences.
The conclusion is both practical and liberating for clinicians: implant material selection in the TA system can be guided by aesthetic and biocompatibility priorities without compromising biomechanical outcomes. Patients who want ceramic implants for the look, the hypoallergenic profile, or the thermal comfort — they can have them, with the same structural confidence.
This matters because the clinical barriers to ceramic implants have historically included uncertainty about stress distribution. The TA’s hyperbolic paraboloid geometry, by distributing forces so efficiently, appears to neutralize the material-specific disadvantages of zirconia at the bone interface — the site that actually determines long-term success.
What the TA System Offers That Conventional Implantology Cannot
For clinicians evaluating whether to engage with this research, the advantages of the TA and DA (Double Abutment) system extend well beyond the biomechanical:
- Rehabilitation of 2–3 element edentulous spans with a single implant — reducing surgical sites, patient morbidity, cost, and healing time
- No welding required — the system is fully passive, eliminating distortion risks introduced by conventional bar or bridge fabrication steps
- Function in inclined implant situations — where traditional systems require parallelism, the TA’s geometry accommodates angulation without compromise
- Elimination of cantilever mechanics — replacing a prosthetic solution known for unfavorable force distribution with one that actively optimizes it
- Natural hygiene compatibility — the parabolic emergence profile of the TA allows conventional dental floss use due to its segmented tripod configuration, supporting patient compliance
- Reduced stress at the implant platform and screw — the primary failure zones in conventional implant-abutment systems are depressurized by the TA’s geometric force dissipation
- Compatible with both ceramic and titanium implants — as confirmed by the 2026 FEA study, without clinically meaningful difference in bone behavior
- Multiple international patents — protecting the design across Brazil, India, Europe, and the United States
It bears stating plainly: this is not a system that asks clinicians to trade outcomes for convenience. The marginal bone loss data across 12 years of follow-up is better than what many conventional single-crown implant studies report. The peri-implant tissue parameters at final examination reflect health, not compromise. And the biomechanical modeling confirms that the forces reaching the bone are within ranges that bone tissue handles well.
Dr. Luciana Colepícolo: The Scientist Behind the Breakthrough
Dr. Luciana Silva Colepícolo
The institutional response to genuinely novel ideas in medicine is rarely swift warmth. When a concept dismantles something that “has always been done this way” — in this case, the fundamental architecture of how implants support prostheses — the default reaction from established voices is often dismissal rather than dialogue.
This is not unique to Dr. Colepícolo’s experience. It is the pattern. And it is why the data matters so much. Not because it should be necessary to prove oneself through a decade of outcomes to earn a fair reading — but because when the data is this good, dismissal without engagement becomes increasingly difficult to sustain as a credible position.
The question for clinicians is not whether this research deserves attention. Twelve years of follow-up data, a peer-reviewed FEA comparison, registration at ClinicalTrials.gov, and ethics committee approval from the Federal University of Minas Gerais — that is not a fringe proposal. That is a body of evidence asking to be read seriously.
What the Research Acknowledges — and Why That Makes It More Credible
Good science is defined partly by its honesty about limitations. Dr. Colepícolo’s team is explicit about the constraints of the current evidence base. The case series, though extraordinary in its follow-up duration and the quality of outcomes documented, is a consecutive case study — not a randomized controlled trial. Radiographic standardization varied between baseline and follow-up due to the time span involved. The FEA study, while methodologically rigorous, uses simplified bone models that cannot fully capture physiological variables like temperature, oral fluids, bruxism, or dynamic masticatory muscle forces.
These are not weaknesses to hide. They are the honest boundaries of a research program at an early-to-intermediate stage — and notably, a research program that has already accumulated more longitudinal clinical data than many widely-adopted implant innovations had at equivalent stages of their development.
What the authors call for — and what the evidence justifies — is the next step: prospective randomized clinical trials comparing TA/DA systems with conventional abutments under controlled conditions. That is how a promising innovation becomes a validated standard of care. The groundwork has been laid. The 12-year data exists. The biomechanical modeling has been done. What is needed now is engagement — from researchers, from clinicians, and from institutions with the resources to run the trials.
To the Dentists Who Haven’t Read the Papers Yet: Here Is Your Invitation
The history of medicine is full of innovations that were laughed at before they were lived with. The idea that Helicobacter pylori causes ulcers. The germ theory of disease. The notion that surgeons should wash their hands. Every one of them met resistance. Every one of them eventually prevailed, not because authority finally approved, but because the evidence accumulated beyond the point where dismissal was intellectually defensible.
Dr. Luciana Colepícolo has not asked for faith. She has published data. She has submitted to peer review. She has registered her clinical study. She has had her biomechanical models independently evaluated. She has followed patients for twelve years and documented the results with radiographs that are published, available, and clear.
The two papers referenced throughout this article are not difficult to find. They are in the peer-reviewed literature. They have reference lists. They have methods sections that describe exactly what was done and exactly what was measured. They are the kind of papers that, once read, make it very hard to return to the posture of dismissal without consequence.
“The proposed TA expands rehabilitation options by enabling the use of a single implant to support multiple crowns — with bone stress values similar between ceramic and titanium models, remaining within acceptable limits.”
Colepícolo et al., International Journal of Medical & Interdisciplinary Research, 2026
Colepícolo et al., International Journal of Medical & Interdisciplinary Research, 2026
For your patients who cannot afford multiple implants but need multiple crowns. For your patients who want ceramic implants but worry about structural performance. For your cases with non-ideal implant angulation. For every situation where conventional implantology forces a compromise, this research deserves your attention.
Read the papers. Look at the radiographs. Engage with the biomechanics. That is all the research has ever asked.
Further Reading
Primary Research References
- Colepícolo LS, Martinez MAM, Cota LOM, Lima RPE, Costa FO. Biomechanical Evaluation of An Innovative Triple Abutment System in Ceramic Versus Titanium Implants: A Finite Element Analysis. International Journal of Medical & Interdisciplinary Research. 2026 Jan;3(1):89–92.
- Colepícolo LS, Martinez MAM, Rodrigues AA, Baeta LS, Costa FO. The innovative double or triple dental abutment-implant: Case study with a 3-to-12-year follow-up. Clinical Advances in Periodontics. 2024. doi: 10.1002/cap
Patents: Brazil BR112020009609A2 · India 517585 · Europe 17932138.5 · USA 11,701,206 B2 | Clinical trial registration: NCT06127576 | Ethics approval: Federal University of Minas Gerais, Approval No. 5895732
The Research Is Published. The Data Is Clear. The Next Step Is Yours.
Read the original papers, share them with your colleagues, and consider what this geometry could mean for your most challenging implant cases.
READY TO JOIN THE REVOLUTION?
Fill in the form by clicking the button below:
This article is a professional editorial summary prepared to support awareness of peer-reviewed research by Dr. Luciana Silva Colepícolo and colleagues at the Federal University of Minas Gerais, Brazil.
All clinical data, statistics, and quotations are drawn directly from the published peer-reviewed papers cited above. No findings have been extrapolated or embellished.
Recent Articles
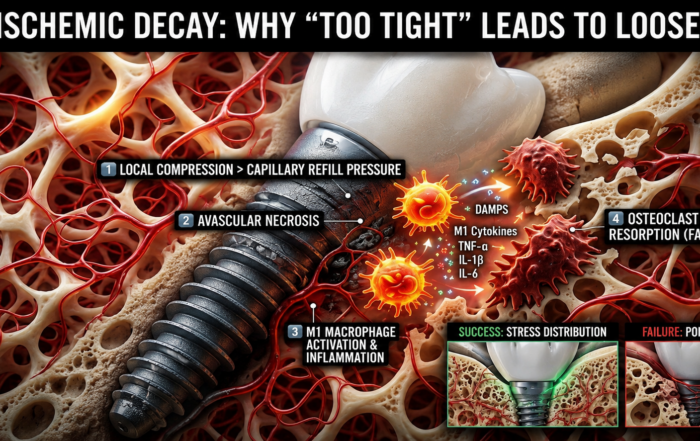
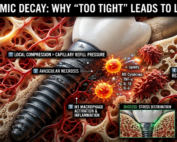
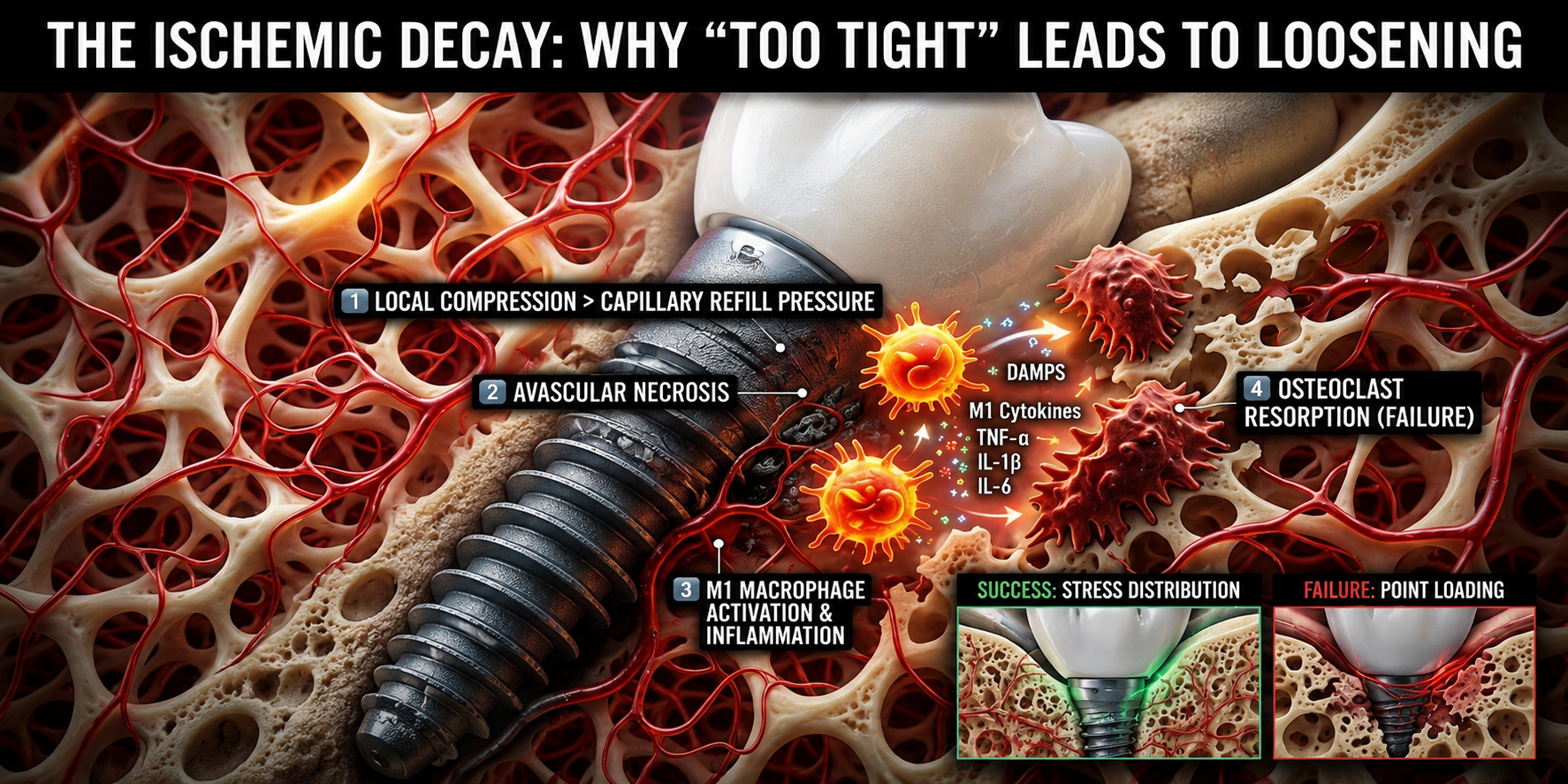
When “Perfectly Tight” Dental Implants Fail
When “Perfectly Tight” Dental Implants Fail The Hidden Role of Ischemic Bone Resorption and Osteoimmune Dysfunction In modern dental implantology, achieving high primary [...]

The Bicuspidization Protocol: Engineering Meets Survival
The Bicuspidization Protocol: Engineering Meets Survival Modern restorative dentistry is no longer limited to extraction and replacement. In the era of conservative and biologically [...]
Pulsed Electromagnetic Field (PEMF) Use in Implant Dentistry
Pulsed Electromagnetic Field (PEMF) Use in Implant Dentistry Abstract and Historical Background Pulsed Electromagnetic Field (PEMF) therapy refers to the application of low-frequency electromagnetic [...]
Laser Therapy in the Management of Peri-Implantitis
Laser Therapy in the Management of Peri-Implantitis Laser technology has become an increasingly valuable adjunct in the treatment of peri-implant diseases, particularly peri-implantitis. Its [...]
Magnetically Guided Dental Nanobots (CalBots) Are Real
Magnetically Guided Dental Nanobots (CalBots) Are Real The concept of nanobots in dentistry has long been associated with futuristic speculation. However, recent peer-reviewed research [...]

Peri-Implantitis Treatment & Prevention Methods
Peri-Implantitis Treatment & Prevention Methods Peri-implantitis remains one of the most significant biological complications affecting dental implants, posing a serious threat to long-term implant [...]

{kind=link}
{kind=link}
{kind=link}