

Dental Biomechanics · Implant Science · Clinical Evidence
Biomechanics of the Triple Abutment & BOPiT Concept
How a saddle-shaped mathematical surface is rewriting the rules of load distribution in implant-supported prosthetics — and why the bone agrees.
Based on peer-reviewed research · Federal University of Minas Gerais, Brazil · 2024–2026
Dental Biomechanics · Implant Science · Clinical Evidence
Biomechanics of the Triple Abutment & BOPiT Concept
How a saddle-shaped mathematical surface is rewriting the rules of load distribution in implant-supported prosthetics — and why the bone agrees.
Based on peer-reviewed research · Federal University of Minas Gerais, Brazil · 2024–2026
Introduction
The Triple Abutment: A New Paradigm in Implant Prosthetics
Every abutment available in implant dentistry today shares a common geometric lineage: the cylinder. Whether the connection is an internal hexagon, an external hexagon, or a Morse taper, the supracrestal prosthetic form of the abutment remains fundamentally the same — a shape optimized for manufacturing convenience rather than biomechanical logic. The consequences have been predictable: stress concentration at the implant platform, bone loss at the abutment junction, and the persistent need for multiple implants to support multiple crowns.
The Triple Abutment (TA), developed by Dr. Luciana Silva Colepícolo at the Federal University of Minas Gerais, Brazil, breaks from this tradition entirely. It is a single prosthetic component, secured to a single osseointegrated implant, capable of supporting two (Double Abutment, DA) or three dental crowns simultaneously. Its design is not derived from convention — it is derived from mathematics, specifically from the geometry of the hyperbolic paraboloid, a doubly-ruled saddle surface with properties that align, with remarkable precision, to the demands of peri-implant biomechanics.
The system is protected by patents in four jurisdictions — Brazil, India, Europe, and the United States — and has been validated through a case series spanning up to 12 years of clinical follow-up, as well as a 2026 finite element analysis comparing ceramic and titanium implant configurations. The results across both bodies of evidence tell the same story: the TA delivers biomechanical performance that conventional abutment systems cannot match.
“The new DA and TA abutments with paraboloid geometric design are totally curved and passive — without welds — and support two or three dental crowns respectively on a single osseointegrated implant, providing biomechanical advantages.”
Colepícolo et al., Clinical Advances in Periodontics, 2024
Crowns supported by a single implant with the Triple Abutment
Maximum years of clinical follow-up documented
Implant success rate across 43 cases
Difference in peri-implant bone stress between ceramic and titanium models

The Science
BOPiT: Biodynamically Optimized Peri-implant Tissue
The Triple Abutment is not merely a geometric innovation — it is the physical expression of a conceptual framework called Biodynamically Optimized Peri-implant Tissue (BOPiT). BOPiT integrates three bodies of scientific knowledge that had not previously been unified in implant abutment design:
The Three Pillars of BOPiT
Bone Mechanotransduction — the biological process by which mechanical signals are converted into biochemical responses at the cellular level. Bone cells are exquisitely sensitive to the pattern, direction, and magnitude of forces delivered to them. The geometry of an abutment determines the character of those signals. Get the geometry right, and bone cells respond with homeostasis. Get it wrong, and they respond with resorption.
Biotensegrity — a biological adaptation of the tensegrity principle from architecture and engineering. Biological structures maintain integrity not through rigid compression but through a dynamic balance of tension and compression distributed across the entire system. The TA’s curved geometry creates a tensegrity-like force distribution that spreads load before it reaches critical tissue interfaces.
Mechanobiology — the study of how physical forces regulate cell behavior, tissue development, and long-term health at the molecular level. BOPiT treats the abutment not as a passive mechanical connector but as an active biological interface — one that shapes the mechanical environment experienced by peri-implant cells throughout the functional life of the prosthesis.
Together, these three principles define what BOPiT proposes: that the geometry of an abutment is a biological signal, not merely a structural feature. The quadric surfaces of the TA allow instantaneous vectorial distribution of received masticatory loads at the implant-abutment connection, with a shift in the center of gravity of the entire assembly — resulting in primary biophysical dissipation of stresses in the abutment before those forces ever reach the bone-implant interface.
This is not an abstract theoretical claim. The observed clinical outcome is a mean annual marginal bone loss of just 0.022 ± 0.05 mm — a figure more commonly associated with pristine natural dentition than with prosthetic implant sites approaching a decade of function.

The Geometry
The Hyperbolic Paraboloid: Mathematics in Service of Biology
The hyperbolic paraboloid — sometimes called a “hypar” — is a doubly-ruled quadric surface: a surface composed entirely of straight lines whose union forms a saddle shape that simultaneously curves upward along one axis and downward along another. This geometry is not unfamiliar to architects and engineers, who have used it for decades in shells and tensile structures precisely because of its structural efficiency.
Why This Shape Works in the Mouth
Masticatory forces are not axial. They arrive at the implant-abutment interface as complex three-dimensional vectors — axial, oblique, shear — in combinations that vary with every chewing cycle. A cylindrical abutment channels all of these forces toward the weakest point: the junction between the abutment and the implant platform, where bone loss classically begins.
The hyperbolic paraboloid geometry of the TA redirects these forces. Because the surface is doubly curved, there is no single axis along which bending stress can concentrate. Forces are decomposed into components that travel along the straight lines of the ruled surface, distributing load across the entire geometry before it reaches the bone. Vectorial loads are minimized, and the traditional axis of transverse coordinates that drives early bone loss at the implant-abutment connection is effectively neutralized.
Critically, the entire system is fully passive. No welding is required. This eliminates one of the most significant sources of error and distortion in conventional multi-unit implant prosthetics, where every welding step introduces potential for dimensional error that compromises passive fit and biomechanical performance.
“Vectorial loads are minimized, preventing the traditional axis of transverse coordinates that imply early bone loss in the implant abutment connection area. These designs represent the interaction that exists between all biological phenomena and mathematics.”
Colepícolo et al., Clinical Advances in Periodontics, 2024
The 2026 finite element analysis confirmed these principles computationally. Under both axial (250 N) and oblique loading (100 N at 45°), bone stress and microstrain differences between ceramic and titanium TA configurations were below 5%, with neither model showing failure regions at the bone interface.

Clinical Advantages
Why the Triple Abutment Changes What Is Possible in Implant Rehabilitation
These are not theoretical benefits — they are outcomes observed and documented across 43 implants in 37 patients, followed for an average of 7.2 years with a maximum of 12 years.
- →Single implant support for 2–3 element spans: Rehabilitates edentulous spaces of 10–20 mm using one osseointegrated implant — eliminating additional surgery, reducing patient morbidity and cost.
- →No welding — fully passive by design: Eliminates framework distortion and all dimensional error introduced at each welding step in conventional prosthetics.
- →Function in non-ideal angulation situations: Works effectively where implant angulation is imperfect, without requiring grafting procedures solely to achieve parallelism.
- →Reduced stress at the implant platform and screw: BOPiT geometry dissipates forces in the abutment before reaching bone — FEA confirmed bone stress differences below 5% across material types.
- →Elimination of cantilever effects: Replaces cantilever bending moments with a geometrically active force-distribution architecture.
- →Natural hygiene compatibility: The parabolic emergence profile allows use of conventional dental floss due to its segmented tripod configuration.
- →Compatible with ceramic and titanium implants equally: Bone stress values differ by less than 5% — implant material choice can be guided by aesthetics and biocompatibility, not biomechanical compromise.
- →Favorable marginal bone loss: Mean annual MBL of 0.022 ± 0.05 mm — far below accepted thresholds, comparing favorably with conventional single-crown implant systems.
Scientific Transparency
Limitations: What the Evidence Does Not Yet Establish
The authors of both publications are explicit and thorough in their acknowledgment of these constraints — and this transparency is itself a mark of scientific credibility.
- →Study design: A consecutive case study, not a randomized controlled trial. Selection bias and the absence of a control group are inherent limitations.
- →Radiographic standardization: Both analog and digital radiographs were used across the 12-year span, introducing some degree of measurement variability.
- →FEA simplifications: Homogeneous and isotropic bone models cannot simulate anisotropic real bone, oral fluids, temperature variation, bruxism, or dynamic masticatory muscle forces.
- →Ceramic loosening risk: Early studies suggest zirconia structures may have inferior resistance to loosening compared to titanium, though surface treatments may mitigate this.
- →Sample size: 43 implants in 37 patients — meaningful for a novel design, but small relative to the scale needed for population-level conclusions.
- →Abutment customization requirement: Each TA must be individually customized to the geometry and inclination of each case, introducing a laboratory dependency beyond conventional abutments.
- →Single-center, single-operator data: All cases were treated by one operator at one center. Reproducibility across different operators and settings has not yet been demonstrated.
These limitations define not the ceiling of what this work has achieved, but the floor of what further research must address.

Looking Ahead
The Future of the Triple Abutment: Where the Research Must Go Next
The groundwork has been laid with uncommon thoroughness. What is needed now is a structured escalation of the evidence base.
- →Prospective randomized clinical trials: Directly comparing the TA and DA with traditional abutments under controlled conditions — the necessary next step toward guideline-level recommendations.
- →Multi-center, multi-operator validation: Demonstrating reproducibility across different clinical settings and operators to establish generalizability.
- →Advanced FEA modeling: Patient-specific bone morphology, anisotropic properties, dynamic loading, and physiological variables — moving toward digital twins of the implant-bone system.
- →Ceramic-specific surface treatment research: Systematic investigation of surface treatments optimized for the TA-zirconia configuration to address the identified loosening concern.
- →Long-term survival curves: Formal Kaplan-Meier and competing risk analysis for direct comparison with published survival data for conventional implant systems.
- →Digital CAD/CAM workflows: The TA’s mathematical precision makes it inherently suited to fully digital design and manufacturing — reducing laboratory customization and improving case-to-case consistency.
- →Overdenture and full-arch applications: Investigation of TA-supported overdentures and full-arch rehabilitation — where single-implant support of multiple elements carries the greatest clinical benefit.
The biomechanical logic is sound. The clinical data is encouraging. The mathematical foundation is precise. What the field now owes this research is the rigor of a full prospective evaluation.

Primary References
Cited Research
- 1.Colepícolo LS, Martinez MAM, Rodrigues AA, Baeta LS, Costa FO. The innovative double or triple dental abutment-implant: Case study with a 3-to-12-year follow-up. Clinical Advances in Periodontics. 2024. © 2024 American Academy of Periodontology.
- 2.Colepícolo LS, Martinez MAM, Cota LOM, Lima RPE, Costa FO. Biomechanical Evaluation of An Innovative Triple Abutment System in Ceramic Versus Titanium Implants: A Finite Element Analysis. International Journal of Medical & Interdisciplinary Research. January 2026;3(1):89–92.
Patents: Brazil BR112020009609A2 · India 517585 · Europe 17932138.5 · USA 11,701,206 B2 | ClinicalTrials.gov: NCT06127576 | Ethics: UFMG No. 5895732
Frequently Asked Questions
10 Clinical Questions Answered from the Published Research
The Triple Abutment (TA) is a prosthetic component designed to support three dental crowns on a single osseointegrated implant. Unlike all conventional abutments — which share a cylindrical geometric design — the TA features a hyperbolic paraboloid geometry that distributes masticatory forces vectorially before they reach the bone-implant interface. The system requires no welding and is fully passive by design.
BOPiT — Biodynamically Optimized Peri-implant Tissue — is the conceptual framework underlying the TA design. It integrates bone mechanotransduction (how bone cells respond to mechanical signals), biotensegrity (dynamic force distribution across biological structures), and mechanobiology (how physical forces regulate cell behavior). BOPiT proposes that abutment geometry is a biological signal that actively shapes the mechanical environment experienced by peri-implant tissues.
43 implants in 37 patients, mean follow-up 7.2 years, maximum 12 years. Key results: mean annual marginal bone loss 0.022 ± 0.05 mm; implant success rate 98%; peri-implant probing depth 3.0 mm at final examination; no statistically significant change in bleeding on probing. Radiographic images showed no angular bone defects or bone craters, with favorable cortical thickness and trabecular mineralization across all cases.
Yes, validated by the 2026 FEA study. Bone stress and microstrain differences between zirconia and titanium TA configurations were below 5% under both axial (250 N) and oblique (100 N at 45°) loading. While the ceramic model showed 10–20% higher stress in prosthetic components due to zirconia’s higher elastic modulus (205 GPa vs 105 GPa for titanium), neither model showed bone-level failure regions. Implant material selection may therefore be guided by aesthetics and biocompatibility, not biomechanical risk.
Zirconia implants offer a whitish, translucent appearance nearly indistinguishable from natural teeth — critical in patients with a thin gingival biotype where metallic grey would compromise the result. They are hypoallergenic (safe for patients with metal sensitivity), have lower thermal conductivity (reducing oral sensitivity), and offer exceptional mechanical resistance (compressive strength ~2000 MPa) with favorable crack-arrest behavior via the martensitic phase transformation mechanism.
The TA rehabilitates edentulous spaces of approximately 20 mm mesiodistally (three-element spans), while the DA addresses approximately 10–15 mm (two-element spans). In the published case series, 88.4% of cases were in the posterior region — the highest functional demand zone — with distribution almost equal between maxilla and mandible. The ability to function in non-ideal implant angulation further extends the range of treatable clinical situations.
Cantilever extensions introduce bending moments that accelerate marginal bone loss and mechanical failure. The TA eliminates the need for cantilevers in two- and three-element posterior spans by providing active multi-crown support from a single implant. As cited in the 2024 paper, while cantilever multi-unit reconstructions show acceptable survival rates, single-implant cantilever data remains insufficient for routine recommendation — a clinical gap the TA directly addresses.
Cylindrical implants with internal hexagon and no surface treatment (Neodent, Grupo Straumann), 4.0 mm diameter, 10 and 13 mm lengths. Notably, the absence of special surface characteristics did not appear to affect outcomes — success rates appeared to relate to force equalization under the abutments rather than implant surface features. This suggests the TA’s biomechanical advantage may compensate for the absence of enhanced osseointegration surfaces, though further comparative study is warranted.
Consecutive case study design (not RCT); variable radiographic standardization over 12 years; FEA models using simplified bone that cannot simulate oral fluids, bruxism, or dynamic forces; small sample (43 implants, 37 patients); all cases treated by a single operator at a single center; abutment customization requirement adds laboratory complexity; and early data suggesting zirconia may have inferior loosening resistance compared to titanium. Future prospective RCTs with multi-center design are explicitly called for by the authors.
The 2026 FEA used 3D models from real CT scans of a dentate maxilla (Type 3 bone), bolt pretensioning (300 N abutment screw, 150 N prosthetic screw), frictional contacts, and both axial and oblique loading. Mesh convergence was verified using second-order tetrahedral elements (736,221 nodes, 441,490 elements). Evaluation criteria included maximum/minimum principal stresses, Von Mises stresses, and strain magnitudes. Equivalent support reactions across both models confirmed correct boundary conditions — meaning the below-5% bone stress differences reflect genuine material behavior, not modeling artifacts.
The Research Is Published. The Data Is Clear. The Next Step Is Yours.
Read the original papers, share them with your colleagues, and consider what this geometry could mean for your most challenging implant cases.
READY TO JOIN THE REVOLUTION?
Fill in the form by clicking the button below:
Recent Articles



































Introduction
The Triple Abutment: A New Paradigm in Implant Prosthetics
Every abutment available in implant dentistry today shares a common geometric lineage: the cylinder. Whether the connection is an internal hexagon, an external hexagon, or a Morse taper, the supracrestal prosthetic form of the abutment remains fundamentally the same — a shape optimized for manufacturing convenience rather than biomechanical logic. The consequences have been predictable: stress concentration at the implant platform, bone loss at the abutment junction, and the persistent need for multiple implants to support multiple crowns.
The Triple Abutment (TA), developed by Dr. Luciana Silva Colepícolo at the Federal University of Minas Gerais, Brazil, breaks from this tradition entirely. It is a single prosthetic component, secured to a single osseointegrated implant, capable of supporting two (Double Abutment, DA) or three dental crowns simultaneously. Its design is not derived from convention — it is derived from mathematics, specifically from the geometry of the hyperbolic paraboloid, a doubly-ruled saddle surface with properties that align, with remarkable precision, to the demands of peri-implant biomechanics.
The system is protected by patents in four jurisdictions — Brazil, India, Europe, and the United States — and has been validated through a case series spanning up to 12 years of clinical follow-up, as well as a 2026 finite element analysis comparing ceramic and titanium implant configurations. The results across both bodies of evidence tell the same story: the TA delivers biomechanical performance that conventional abutment systems cannot match.
“The new DA and TA abutments with paraboloid geometric design are totally curved and passive — without welds — and support two or three dental crowns respectively on a single osseointegrated implant, providing biomechanical advantages.”
Colepícolo et al., Clinical Advances in Periodontics, 2024
Crowns supported by a single implant with the Triple Abutment
Maximum years of clinical follow-up documented
Implant success rate across 43 cases
Difference in peri-implant bone stress between ceramic and titanium models
The Science
BOPiT: Biodynamically Optimized Peri-implant Tissue
The Triple Abutment is not merely a geometric innovation — it is the physical expression of a conceptual framework called Biodynamically Optimized Peri-implant Tissue (BOPiT). BOPiT integrates three bodies of scientific knowledge that had not previously been unified in implant abutment design:
The Three Pillars of BOPiT
Bone Mechanotransduction — the biological process by which mechanical signals are converted into biochemical responses at the cellular level. Bone cells are exquisitely sensitive to the pattern, direction, and magnitude of forces delivered to them. The geometry of an abutment determines the character of those signals. Get the geometry right, and bone cells respond with homeostasis. Get it wrong, and they respond with resorption.
Biotensegrity — a biological adaptation of the tensegrity principle from architecture and engineering. Biological structures maintain integrity not through rigid compression but through a dynamic balance of tension and compression distributed across the entire system. The TA’s curved geometry creates a tensegrity-like force distribution that spreads load before it reaches critical tissue interfaces.
Mechanobiology — the study of how physical forces regulate cell behavior, tissue development, and long-term health at the molecular level. BOPiT treats the abutment not as a passive mechanical connector but as an active biological interface — one that shapes the mechanical environment experienced by peri-implant cells throughout the functional life of the prosthesis.
Together, these three principles define what BOPiT proposes: that the geometry of an abutment is a biological signal, not merely a structural feature. The quadric surfaces of the TA allow instantaneous vectorial distribution of received masticatory loads at the implant-abutment connection, with a shift in the center of gravity of the entire assembly — resulting in primary biophysical dissipation of stresses in the abutment before those forces ever reach the bone-implant interface.
This is not an abstract theoretical claim. The observed clinical outcome is a mean annual marginal bone loss of just 0.022 ± 0.05 mm — a figure more commonly associated with pristine natural dentition than with prosthetic implant sites approaching a decade of function.
The Geometry
The Hyperbolic Paraboloid: Mathematics in Service of Biology
The hyperbolic paraboloid — sometimes called a “hypar” — is a doubly-ruled quadric surface: a surface composed entirely of straight lines whose union forms a saddle shape that simultaneously curves upward along one axis and downward along another. This geometry is not unfamiliar to architects and engineers, who have used it for decades in shells and tensile structures precisely because of its structural efficiency.
Why This Shape Works in the Mouth
Masticatory forces are not axial. They arrive at the implant-abutment interface as complex three-dimensional vectors — axial, oblique, shear — in combinations that vary with every chewing cycle. A cylindrical abutment channels all of these forces toward the weakest point: the junction between the abutment and the implant platform, where bone loss classically begins.
The hyperbolic paraboloid geometry of the TA redirects these forces. Because the surface is doubly curved, there is no single axis along which bending stress can concentrate. Forces are decomposed into components that travel along the straight lines of the ruled surface, distributing load across the entire geometry before it reaches the bone. Vectorial loads are minimized, and the traditional axis of transverse coordinates that drives early bone loss at the implant-abutment connection is effectively neutralized.
Critically, the entire system is fully passive. No welding is required. This eliminates one of the most significant sources of error and distortion in conventional multi-unit implant prosthetics, where every welding step introduces potential for dimensional error that compromises passive fit and biomechanical performance.
“Vectorial loads are minimized, preventing the traditional axis of transverse coordinates that imply early bone loss in the implant abutment connection area. These designs represent the interaction that exists between all biological phenomena and mathematics.”
Colepícolo et al., Clinical Advances in Periodontics, 2024
The 2026 finite element analysis confirmed these principles computationally. Under both axial (250 N) and oblique loading (100 N at 45°), bone stress and microstrain differences between ceramic and titanium TA configurations were below 5%, with neither model showing failure regions at the bone interface.
Clinical Advantages
Why the Triple Abutment Changes What Is Possible in Implant Rehabilitation
These are not theoretical benefits — they are outcomes observed and documented across 43 implants in 37 patients, followed for an average of 7.2 years with a maximum of 12 years.
- →Single implant support for 2–3 element spans: Rehabilitates edentulous spaces of 10–20 mm using one osseointegrated implant — eliminating additional surgery, reducing patient morbidity and cost.
- →No welding — fully passive by design: Eliminates framework distortion and all dimensional error introduced at each welding step in conventional prosthetics.
- →Function in non-ideal angulation situations: Works effectively where implant angulation is imperfect, without requiring grafting procedures solely to achieve parallelism.
- →Reduced stress at the implant platform and screw: BOPiT geometry dissipates forces in the abutment before reaching bone — FEA confirmed bone stress differences below 5% across material types.
- →Elimination of cantilever effects: Replaces cantilever bending moments with a geometrically active force-distribution architecture.
- →Natural hygiene compatibility: The parabolic emergence profile allows use of conventional dental floss due to its segmented tripod configuration.
- →Compatible with ceramic and titanium implants equally: Bone stress values differ by less than 5% — implant material choice can be guided by aesthetics and biocompatibility, not biomechanical compromise.
- →Favorable marginal bone loss: Mean annual MBL of 0.022 ± 0.05 mm — far below accepted thresholds, comparing favorably with conventional single-crown implant systems.
Scientific Transparency
Limitations: What the Evidence Does Not Yet Establish
The authors of both publications are explicit and thorough in their acknowledgment of these constraints — and this transparency is itself a mark of scientific credibility.
- →Study design: A consecutive case study, not a randomized controlled trial. Selection bias and the absence of a control group are inherent limitations.
- →Radiographic standardization: Both analog and digital radiographs were used across the 12-year span, introducing some degree of measurement variability.
- →FEA simplifications: Homogeneous and isotropic bone models cannot simulate anisotropic real bone, oral fluids, temperature variation, bruxism, or dynamic masticatory muscle forces.
- →Ceramic loosening risk: Early studies suggest zirconia structures may have inferior resistance to loosening compared to titanium, though surface treatments may mitigate this.
- →Sample size: 43 implants in 37 patients — meaningful for a novel design, but small relative to the scale needed for population-level conclusions.
- →Abutment customization requirement: Each TA must be individually customized to the geometry and inclination of each case, introducing a laboratory dependency beyond conventional abutments.
- →Single-center, single-operator data: All cases were treated by one operator at one center. Reproducibility across different operators and settings has not yet been demonstrated.
These limitations define not the ceiling of what this work has achieved, but the floor of what further research must address.
Looking Ahead
The Future of the Triple Abutment: Where the Research Must Go Next
The groundwork has been laid with uncommon thoroughness. What is needed now is a structured escalation of the evidence base.
- →Prospective randomized clinical trials: Directly comparing the TA and DA with traditional abutments under controlled conditions — the necessary next step toward guideline-level recommendations.
- →Multi-center, multi-operator validation: Demonstrating reproducibility across different clinical settings and operators to establish generalizability.
- →Advanced FEA modeling: Patient-specific bone morphology, anisotropic properties, dynamic loading, and physiological variables — moving toward digital twins of the implant-bone system.
- →Ceramic-specific surface treatment research: Systematic investigation of surface treatments optimized for the TA-zirconia configuration to address the identified loosening concern.
- →Long-term survival curves: Formal Kaplan-Meier and competing risk analysis for direct comparison with published survival data for conventional implant systems.
- →Digital CAD/CAM workflows: The TA’s mathematical precision makes it inherently suited to fully digital design and manufacturing — reducing laboratory customization and improving case-to-case consistency.
- →Overdenture and full-arch applications: Investigation of TA-supported overdentures and full-arch rehabilitation — where single-implant support of multiple elements carries the greatest clinical benefit.
The biomechanical logic is sound. The clinical data is encouraging. The mathematical foundation is precise. What the field now owes this research is the rigor of a full prospective evaluation.
Primary References
Cited Research
- 1.Colepícolo LS, Martinez MAM, Rodrigues AA, Baeta LS, Costa FO. The innovative double or triple dental abutment-implant: Case study with a 3-to-12-year follow-up. Clinical Advances in Periodontics. 2024. © 2024 American Academy of Periodontology.
- 2.Colepícolo LS, Martinez MAM, Cota LOM, Lima RPE, Costa FO. Biomechanical Evaluation of An Innovative Triple Abutment System in Ceramic Versus Titanium Implants: A Finite Element Analysis. International Journal of Medical & Interdisciplinary Research. January 2026;3(1):89–92.
Patents: Brazil BR112020009609A2 · India 517585 · Europe 17932138.5 · USA 11,701,206 B2 | ClinicalTrials.gov: NCT06127576 | Ethics: UFMG No. 5895732
Frequently Asked Questions
10 Clinical Questions Answered from the Published Research
The Triple Abutment (TA) is a prosthetic component designed to support three dental crowns on a single osseointegrated implant. Unlike all conventional abutments — which share a cylindrical geometric design — the TA features a hyperbolic paraboloid geometry that distributes masticatory forces vectorially before they reach the bone-implant interface. The system requires no welding and is fully passive by design.
BOPiT — Biodynamically Optimized Peri-implant Tissue — is the conceptual framework underlying the TA design. It integrates bone mechanotransduction (how bone cells respond to mechanical signals), biotensegrity (dynamic force distribution across biological structures), and mechanobiology (how physical forces regulate cell behavior). BOPiT proposes that abutment geometry is a biological signal that actively shapes the mechanical environment experienced by peri-implant tissues.
43 implants in 37 patients, mean follow-up 7.2 years, maximum 12 years. Key results: mean annual marginal bone loss 0.022 ± 0.05 mm; implant success rate 98%; peri-implant probing depth 3.0 mm at final examination; no statistically significant change in bleeding on probing. Radiographic images showed no angular bone defects or bone craters, with favorable cortical thickness and trabecular mineralization across all cases.
Yes, validated by the 2026 FEA study. Bone stress and microstrain differences between zirconia and titanium TA configurations were below 5% under both axial (250 N) and oblique (100 N at 45°) loading. While the ceramic model showed 10–20% higher stress in prosthetic components due to zirconia’s higher elastic modulus (205 GPa vs 105 GPa for titanium), neither model showed bone-level failure regions. Implant material selection may therefore be guided by aesthetics and biocompatibility, not biomechanical risk.
Zirconia implants offer a whitish, translucent appearance nearly indistinguishable from natural teeth — critical in patients with a thin gingival biotype where metallic grey would compromise the result. They are hypoallergenic (safe for patients with metal sensitivity), have lower thermal conductivity (reducing oral sensitivity), and offer exceptional mechanical resistance (compressive strength ~2000 MPa) with favorable crack-arrest behavior via the martensitic phase transformation mechanism.
The TA rehabilitates edentulous spaces of approximately 20 mm mesiodistally (three-element spans), while the DA addresses approximately 10–15 mm (two-element spans). In the published case series, 88.4% of cases were in the posterior region — the highest functional demand zone — with distribution almost equal between maxilla and mandible. The ability to function in non-ideal implant angulation further extends the range of treatable clinical situations.
Cantilever extensions introduce bending moments that accelerate marginal bone loss and mechanical failure. The TA eliminates the need for cantilevers in two- and three-element posterior spans by providing active multi-crown support from a single implant. As cited in the 2024 paper, while cantilever multi-unit reconstructions show acceptable survival rates, single-implant cantilever data remains insufficient for routine recommendation — a clinical gap the TA directly addresses.
Cylindrical implants with internal hexagon and no surface treatment (Neodent, Grupo Straumann), 4.0 mm diameter, 10 and 13 mm lengths. Notably, the absence of special surface characteristics did not appear to affect outcomes — success rates appeared to relate to force equalization under the abutments rather than implant surface features. This suggests the TA’s biomechanical advantage may compensate for the absence of enhanced osseointegration surfaces, though further comparative study is warranted.
Consecutive case study design (not RCT); variable radiographic standardization over 12 years; FEA models using simplified bone that cannot simulate oral fluids, bruxism, or dynamic forces; small sample (43 implants, 37 patients); all cases treated by a single operator at a single center; abutment customization requirement adds laboratory complexity; and early data suggesting zirconia may have inferior loosening resistance compared to titanium. Future prospective RCTs with multi-center design are explicitly called for by the authors.
The 2026 FEA used 3D models from real CT scans of a dentate maxilla (Type 3 bone), bolt pretensioning (300 N abutment screw, 150 N prosthetic screw), frictional contacts, and both axial and oblique loading. Mesh convergence was verified using second-order tetrahedral elements (736,221 nodes, 441,490 elements). Evaluation criteria included maximum/minimum principal stresses, Von Mises stresses, and strain magnitudes. Equivalent support reactions across both models confirmed correct boundary conditions — meaning the below-5% bone stress differences reflect genuine material behavior, not modeling artifacts.
The Research Is Published. The Data Is Clear. The Next Step Is Yours.
Read the original papers, share them with your colleagues, and consider what this geometry could mean for your most challenging implant cases.
READY TO JOIN THE REVOLUTION?
Fill in the form by clicking the button below:
Recent Articles

The Woman Who Proved One Implant Could Hold Three Crowns
The Woman Who Proved One Implant Could Hold Three Crowns While the dental establishment looked away, Dr. Luciana Colepícolo spent 12 years building the [...]
ENPP1, The Molecular Brake That Limits Tissue Healing
ENPP1, The Molecular Brake That Limits Tissue Healing Introduction: A New Biological Barrier to Dental Regeneration Meet ENPP1—a protein most dentists have never heard [...]
The Rise of Self‑Healing Dental Biomaterials
The Rise of Self‑Healing Dental Biomaterials Introduction In modern restorative dentistry, durability and longevity of materials remain among the greatest clinical challenges. Traditional dental [...]

Water Fluoridation and IQ Scores in Offspring
Water Fluoridation and IQ Scores in Offspring Community water fluoridation has long been regarded as one of the most effective public health interventions for [...]
Dental X-Rays and Brain Tumors
Dental X-Rays and Brain Tumors Dental radiography is a cornerstone of modern dentistry, enabling clinicians to diagnose caries, periodontal disease, and periapical pathology with [...]
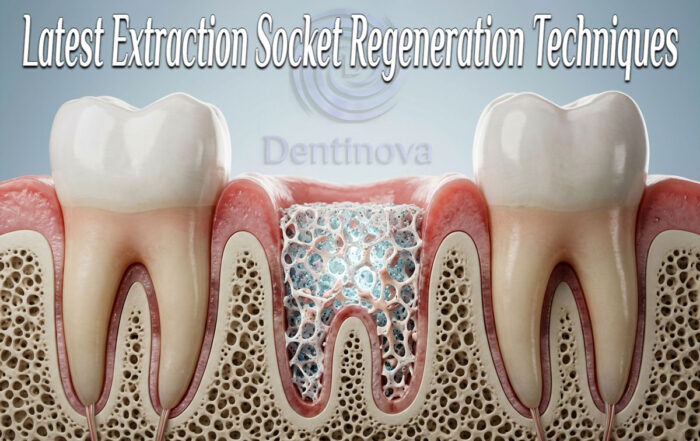
Latest Extraction Socket Regeneration Techniques
Latest Extraction Socket Regeneration Techniques Introduction The alveolar bone surrounding a tooth is a highly specialized structure characterized by a distinctive microarchitecture. One of [...]

{kind=link}
{kind=link}
{kind=link}