

ENPP1, The Molecular Brake That Limits Tissue Healing
Introduction: A New Biological Barrier to Dental Regeneration
Meet ENPP1—a protein most dentists have never heard of, yet one that may be silently undermining your best work.
For decades, dentistry has operated on a repair-and-replace model. We clean, fill, extract, and implant, masterfully treating the consequences of failed healing rather than the root cause. But what if the problem wasn’t the technique, the material, or the patient’s compliance? What if something inside the body was actively slamming the brakes on regeneration?
Originally discovered in cardiac research, ENPP1 acts like a molecular guard dog, blocking the metabolic pathways tissues need to rebuild themselves. And here’s the kicker: it operates in the very same tissues you work with every day—dental pulp, periodontal ligament, alveolar bone, and gingival connective tissue.
This isn’t just basic science. It’s a paradigm shift. The future of regenerative dentistry isn’t about adding more membranes, growth factors, or grafts. It’s about removing the invisible biological barriers already inside your patient.
And that changes everything.
The Silent Saboteur Inside Every Wound
Let me introduce you to a protein you’ve probably never heard of—but one that may be quietly undermining your patients’ healing, case after case.
Its name is ENPP1. And it lives on the surface of cells. Specifically, the very cells you deal with daily: fibroblasts, inflammatory cells, and endothelial cells. In other words, the building blocks of every surgical site you create.
So what does ENPP1 actually do?
Think of it as a metabolic hijacker.
Under normal conditions, injured cells release ATP—a powerful danger signal that screams, “Heal here!” ATP is supposed to kickstart regeneration. But ENPP1 has other plans.
This enzyme grabs that ATP and shreds it. Converts it into AMP. A single, seemingly small chemical change.
And yet, that tiny shift changes everything.
Because AMP doesn’t send the same “heal now” signal. Instead, the cellular engine sputters. Energy drops. The machinery of regeneration—cell division, new blood vessel growth, collagen production, stem cell activation—all of it slows to a crawl.
ENPP1 doesn’t just appear randomly. It becomes highly expressed exactly where you don’t want it—in injured oral tissues. After pulp exposure. After an extraction. Right around that fresh implant site you so carefully prepared.
So while you’re doing everything right surgically, ENPP1 may be quietly transforming a pro-healing environment into a metabolically suppressed one.
A silent saboteur, working beneath the surface.
Now that you know it’s there… the real question is: what can we do about it?
The Moment Healing Breaks: A Step-by-Step Betrayal
Picture this. A patient sits in your chair with deep caries approaching the pulp. Or perhaps you’ve just completed a periodontal flap, and everything looks textbook perfect. You’ve done your job. Now, you trust the body to do its job.
But inside that wound, invisible and silent, a betrayal is about to unfold.
Let me walk you through exactly how ENPP1 hijacks the healing process, step by step. Because understanding this cascade is the first step to stopping it.
Act One: The Injury
Tissue is damaged. Maybe from decay. Maybe from your surgical instruments. Either way, cells rupture. And as they die, they scream for help, by flooding the area with ATP. This is nature’s emergency broadcast system. It means: “Heal here. Now.”
Act Two: The Saboteur Arrives
Enter ENPP1. The enzyme doesn’t warn. It doesn’t negotiate. It simply goes to work, grabbing every ATP molecule it can find and converting it into AMP.
At first glance? Just chemistry. No big deal.
But here’s where the story turns dark.
Act Three: The Domino Effect
That newly formed AMP doesn’t just sit there. It signals neighboring cells—odontoblast-like cells, fibroblasts, the very cells you need for repair—to release two specific substances: adenine and purine nucleosides.
Innocent names. Devastating consequences.
Because those molecules do one thing exceptionally well: they shut down pyrimidine biosynthesis.
Act Four: The Collapse
Pyrimidines are the building blocks of DNA. No pyrimidines? No DNA replication. No DNA replication? No new cells. No new cells? No healing.
The clinical toll is brutal:
Fibroblasts stop multiplying, so connective tissue never forms properly
Endothelial cells die off, so new blood vessels never arrive to feed the wound
Angiogenesis grinds to a halt, so oxygen and nutrients can’t reach the site
And finally, p53-mediated pathways trigger widespread apoptosis, programmed cell death
What This Means for Your Patients
In dental terms? Let me translate.
That pulp exposure you’re trying to cap? Slower healing. Poor outcomes.
That periodontal defect you carefully grafted? Regeneration fails. Scar tissue forms instead of true repair.
That extraction socket you hoped would remodel beautifully? Fibrosis. Not healing.
ENPP1 doesn’t just slow things down. It actively changes the quality of repair, replacing regeneration with scar.
And until now, you’ve had no way to stop it.
But that’s about to change.
From the Heart to Your Chair: A Cardiac Discovery Changes Regenerative Dentistry
Let me pause for a moment. You might be thinking: “This is fascinating, but I treat teeth and gums—not heart attacks.”
Fair question. Here’s the surprising answer.
The original research on ENPP1 came from cardiac injury models. Scientists were trying to understand why some hearts heal poorly after a heart attack. And what they found was this same molecular brake,” ENPP1″, quietly sabotaging regeneration.
But here’s where the story gets personal for you.
The tissues ENPP1 attacks in the heart? Fibroblasts. Endothelial cells. Inflammatory cells. Healing pathways? ATP metabolism. Pyrimidine synthesis. Cell proliferation.
Sound familiar?
Those aren’t heart cells. Those are your cells. The same ones you depend on every single day to heal pulp, periodontium, bone, and gingiva.
Let me walk you through four scenarios you’ve likely faced this week—and show you exactly where ENPP1 has been hiding in plain sight.
1. The Pulp Cap That Failed for No Good Reason
You’ve seen it. A deep caries excavation. Direct pulp cap. Beautiful protocol. And six weeks later? No dentin bridge. Worse—the tooth needs root canal therapy.
You blamed yourself. Maybe the contamination. Maybe the material.
But consider this: ENPP1-induced metabolic disruption may have silently limited stem cell proliferation in that pulp. No proliferation? No differentiation. No dentin bridge. Just necrosis waiting to happen.
2. The Periodontal Case That Never Quite Healed
You did everything right. Flap. Debridement. Graft. Membrane. The patient complied perfectly. And yet, six months later? Attachment gain was disappointing. The defect filled with scar, not bone.
ENPP1 attacks the three cell types you needed most: fibroblasts, osteoblasts, and endothelial cells. All three. Simultaneously. The result? Fibrotic repair instead of true regeneration. Reduced attachment. A clinical failure that wasn’t your fault.
3. The Implant That Took Forever to Integrate
Some implants just feel different, don’t they? Primary stability was good. The patient healed slowly. Integration took months longer than expected. Bone quality on follow-up? Suboptimal.
Osseointegration demands rapid bone remodeling and robust vascularization. ENPP1 overactivity chokes both. Delayed integration. Poor bone quality. An implant at risk—before it even sees a crown.
4. The Extraction Socket That Healed Ugly
Simple extraction. Healthy patient. And yet, the socket filled with soft, scar-like tissue instead of beautiful, ridge-forming bone. The future implant site? Compromised before you started.
ENPP1 promotes inflammation. Slows cell turnover. And worst of all, favors scar over bone. Exactly what you don’t want in an extraction site.
This isn’t theoretical. These aren’t lab-bench curiosities. These are your Monday mornings. Your failed pulp caps. Your sluggish periodontals. Your slow implants. Your ugly sockets.
ENPP1 has been there all along.
Now that you know its name… let’s talk about what you can do about it.
The Wrong Question We’ve Been Asking for Decades
Stop for a moment and think about how we practice regenerative dentistry today.
We take a surgical site—say, a periodontal defect or an extraction socket—and what do we do? We pour in growth factors. Pack it with biomaterials. Sometimes even transplant stem cells.
The underlying assumption has always been the same: healing fails because something is missing.
So we add more. More BMPs. More scaffolds. More cells. More, more, more.
And yet, cases still fail. Pulps don’t cap. Implants don’t integrate. Periodontal defects scar instead of regenerate.
Maybe—just maybe—we’ve been asking the wrong question all along.
What If the Problem Isn’t Absence, but Presence?
Here’s what the ENPP1 model taught us, and it changes everything.
What if healing fails not because something is missing—but because something is actively blocking the process?
Think of it like this. You’re trying to drive a car. The engine won’t start. So you keep adding more fuel. More air. More spark.
But the real problem? Someone left the parking brake on.
ENPP1 is that parking brake.
And no amount of growth factors will overcome a brake that’s fully engaged.
The Shift: From Adding to Removing
This is the paradigm shift I want you to walk away with today.
| Traditional Approach | ENPP1-Based Approach |
|---|---|
| Force regeneration | Remove inhibition |
| Add growth factors | Block ENPP1 activity |
| Overstimulate cells | Restore normal metabolism |
| Fight the wound | Let the body heal itself |
Which one sounds more elegant to you?
Instead of pushing tissues uphill against a molecular brake, we simply release the brake—and let the body’s own remarkable repair machinery do what it evolved to do.
This isn’t theoretical. The biology is already there, inside every patient. We just have to stop sabotaging it.
Three Ways to Release the Brake—Today and Tomorrow
So how do we actually do this? Researchers have identified three distinct strategies. Two are still on the horizon. One is surprisingly simple.
Strategy 1: ENPP1 Inhibitors or Anti-ENPP1 (Coming Soon)
Small molecule inhibitors exist right now. Flavonoid-based compounds like myricetin have already shown they can reduce cell death and improve tissue repair.
Imagine walking into your operatory five years from now and reaching for:
A post-surgical healing gel that blocks ENPP1 at the extraction site
An implant surface coating that releases inhibitor directly into the bone
An endodontic medicament that protects the pulp during vital therapy
Not science fiction. Just smart pharmacology.
Strategy 2: Monoclonal Antibodies (The Precision Strike)
For more targeted cases, we could use antibodies that bind ENPP1 directly—neutralizing it like a guided missile.
The dental applications are breathtaking:
An injectable therapy for a stubborn periodontal defect
An adjunct injection during regenerative endodontics
A local shot at the time of implant placement
No systemic side effects. No off-target issues. Just a precise removal of the brake, exactly where you need it.
Strategy 3: Pyrimidine Supplementation (The Elegant Surprise)
And now, let me share the most compelling finding of all.
Remember how ENPP1 shuts down pyrimidine biosynthesis—the very building blocks of DNA? What if we simply gave those building blocks back?
Researchers tried exactly that. With a simple, natural molecule called uridine.
The results were stunning. Uridine supplementation restored pyrimidine balance. Prevented DNA damage. Rescued healing completely.
In dental terms:
A nutritional adjunct patients could take before and after surgery
A local delivery system mixed into your bone graft material
A simple, low-cost way to support regeneration from the inside out
For decades, we’ve been forcing growth. Adding more. Pushing harder.
The ENPP1 model offers something better: remove the brake, step back, and let the body do what it already knows how to do.
That’s not just a new technique. That’s a new philosophy.
And it might just change the way you treat your next patient.
The Question You’ve Asked Yourself a Hundred Times
Haven’t you ever had a case that should have healed perfectly, but didn’t?
Clean surgery. Healthy patient. Good materials. Perfect technique. And yet, the regeneration failed. The pulp necrosed. The implant lagged. The socket filled with scar instead of bone.
You replayed every step. You couldn’t find your mistake. Because there wasn’t one.
For years, we’ve called these “unpredictable outcomes.” A polite way of saying: we don’t know why.
But what if I told you that ENPP1 just handed you the missing explanation?
The Real Reason Some Cases Fail (Hint: It’s Not Your Technique)
Let me reframe everything you just learned into one clear, clinical truth:
Healing failure isn’t always about infection, poor blood supply, or surgical error.
Sometimes, it’s metabolic.
ENPP1 creates three specific, measurable problems inside a healing wound:
Metabolic imbalance: The ATP-to-AMP shift starves cells of the energy they need to rebuild.
Loss of proliferative capacity: Fibroblasts, osteoblasts, and stem cells stop multiplying.
DNA damage: Without pyrimidines, regenerating tissues literally cannot copy their genetic code.
That’s not a technique failure. That’s biology slamming the brakes.
And once you understand that, your diagnostic perspective shifts forever. You stop asking only “What did I do wrong?” and start asking “Was the metabolic brake engaged?”
Where Do We Go From Here? The Next Decade of Dentistry
The discovery of ENPP1 isn’t just a footnote in a biochemistry journal. It’s a roadmap. Here is where this road leads.
1. Metabolic Modulation
The future dentist won’t just clean and fill. They will manage cellular metabolism. Small molecules, local delivery systems, and targeted inhibitors will become as common as local anesthetics.
2. Precision Regenerative Therapy
Imagine this: you take a small tissue sample from a chronic periodontal defect. A chairside test measures ENPP1 activity. You then customize the treatment—more inhibitor, more uridine, or both—specifically for that patient, that site, that wound.
Not one-size-fits-all. Precision healing.
3. Combination Therapies
Why choose between growth factors and ENPP1 inhibitors? The future is both.
Biomaterials to scaffold the wound
Growth factors to stimulate cells
ENPP1 inhibitors to release the brake
Three tools. One goal. Unstoppable regeneration.
4. Chairside Biological Interventions
No waiting for labs. No systemic medications. Just a syringe, a gel, or a coating applied during the procedure. Rapid. Localized. Powerful.
You place the implant. You coat it with an ENPP1 inhibitor. You close.
And for the first time, you know you’ve removed the hidden barrier to healing.
A New Frontier: Removing the Invisible Hand Brake
Let me leave you with this.
For decades, regenerative dentistry has been a story of addition. Add growth factors. Add cells. Add scaffolds. Push harder.
ENPP1 tells us a different story. A better one.
Healing is not always limited by lack of stimulation.
Sometimes, it is limited by active biological suppression.
Think about the power of that sentence.
It means that inside every wound that failed to heal, there wasn’t a deficit of healing signals. There was a blockade.
And now, for the first time, we know how to remove it.
The Gateway to True Regeneration
ENPP1 is not just another protein. It’s not a footnote. It’s not a lab curiosity.
It is a gateway.
A gateway to faster healing. More predictable regeneration. Biologically optimized outcomes.
For you, the clinician, it means fewer sleepless nights wondering why a good case went bad.
For your patients, it means wounds that truly heal. Pulps that regenerate. Implants that integrate. Sockets that become bone.
The brake has a name now. ENPP1.
And now that you know its name… you know exactly what to do.
Frequently Asked Questions (FAQ) About ENPP1
1. What is ENPP1 in simple terms?
ENPP1 is an enzyme found on the surface of cells that regulates how energy molecules like ATP are used outside the cell. In the context of healing, it acts like a biological “brake”, reducing the signals that normally promote tissue repair and regeneration.
2. Why is ENPP1 important in dental treatments?
ENPP1 directly affects how well oral tissues heal after procedures such as fillings, root canals, implants, or extractions. High ENPP1 activity can:
- Slow down tissue regeneration
- Reduce blood vessel formation
- Increase the risk of incomplete healing
This makes it a key factor in determining treatment success or failure.
3. Does ENPP1 affect dental implants?
Yes, potentially. Successful implant integration depends on strong bone healing and vascularization. Elevated ENPP1 activity may:
- Delay bone formation
- Reduce implant stability over time
- Contribute to early implant failure in some cases
This is why targeting ENPP1 could improve osseointegration outcomes in the future.
4. Can ENPP1 impact root canal or pulp treatments?
Absolutely. In procedures like vital pulp therapy or regenerative endodontics, healing relies on stem cell activity and dentin formation. ENPP1 may:
- Inhibit stem cell proliferation
- Reduce dentin bridge formation
- Increase the likelihood of pulp necrosis
Controlling ENPP1 could significantly improve pulp preservation strategies.
5. Are there treatments available now that target ENPP1?
Currently, ENPP1-targeted therapies are still in the research and experimental stage. However, promising approaches include:
- Small molecule inhibitors
- Monoclonal antibodies
- Metabolic support therapies مثل uridine
These may become part of clinical dentistry in the near future.
6. How could dentists use ENPP1 inhibition in practice?
In the future, dentists might apply ENPP1-targeting therapies through:
- Local gels or medicaments after surgery
- Coatings on dental implants
- Additives in bone graft materials
The goal would be to enhance natural healing rather than forcing it.
7. Does ENPP1 explain why some patients heal slower than others?
It could be one of the key reasons. Variations in ENPP1 expression or activity may lead to:
- Slower cell regeneration
- Increased inflammation
- Higher risk of fibrosis instead of true healing
This supports the idea of personalized dentistry based on molecular biology.
8. Is ENPP1 related to inflammation or infection?
Indirectly, yes. ENPP1 is activated during tissue injury and inflammation. While it does not cause infection, it can:
- Prolong inflammatory responses
- Reduce the efficiency of tissue repair
This makes it an important link between inflammation and impaired healing.
9. What is the future of ENPP1 research in dentistry?
Research is moving toward integrating ENPP1 modulation into regenerative protocols, including:
- Stem cell therapies
- Tissue engineering
- Advanced biomaterials
In the long term, controlling ENPP1 could become a standard component of advanced dental care.
Reference:
Cardiomyocytes disrupt pyrimidine biosynthesis in nonmyocytes to regulate heart repair
Shen Li, Tomohiro Yokota, Ping Wang, Johanna ten Hoeve, Feiyang Ma, Thuc M. Le, Evan R. Abt, Yonggang Zhou, Rimao Wu, Maxine Nanthavongdouangsy, Abraham Rodriguez, Yijie Wang, Yen-Ju Lin, Hayato Muranaka, Mark Sharpley, Demetrios T. Braddock, Vicky E. MacRae, Utpal Banerjee, Pei-Yu Chiou, Marcus Seldin, Dian Huang, Michael Teitell, Ilya Gertsman, Michael Jung, Steven J. Bensinger, Robert Damoiseaux, Kym Faull, Matteo Pellegrini, Aldons J. Lusis, Thomas G. Graeber, Caius G. Radu, and Arjun Deb.
Recent Articles























Follow Us









Introduction: A New Biological Barrier to Dental Regeneration
Meet ENPP1—a protein most dentists have never heard of, yet one that may be silently undermining your best work.
For decades, dentistry has operated on a repair-and-replace model. We clean, fill, extract, and implant, masterfully treating the consequences of failed healing rather than the root cause. But what if the problem wasn’t the technique, the material, or the patient’s compliance? What if something inside the body was actively slamming the brakes on regeneration?
Originally discovered in cardiac research, ENPP1 acts like a molecular guard dog, blocking the metabolic pathways tissues need to rebuild themselves. And here’s the kicker: it operates in the very same tissues you work with every day—dental pulp, periodontal ligament, alveolar bone, and gingival connective tissue.
This isn’t just basic science. It’s a paradigm shift. The future of regenerative dentistry isn’t about adding more membranes, growth factors, or grafts. It’s about removing the invisible biological barriers already inside your patient.
And that changes everything.
The Silent Saboteur Inside Every Wound
Let me introduce you to a protein you’ve probably never heard of—but one that may be quietly undermining your patients’ healing, case after case.
Its name is ENPP1. And it lives on the surface of cells. Specifically, the very cells you deal with daily: fibroblasts, inflammatory cells, and endothelial cells. In other words, the building blocks of every surgical site you create.
So what does ENPP1 actually do?
Think of it as a metabolic hijacker.
Under normal conditions, injured cells release ATP—a powerful danger signal that screams, “Heal here!” ATP is supposed to kickstart regeneration. But ENPP1 has other plans.
This enzyme grabs that ATP and shreds it. Converts it into AMP. A single, seemingly small chemical change.
And yet, that tiny shift changes everything.
Because AMP doesn’t send the same “heal now” signal. Instead, the cellular engine sputters. Energy drops. The machinery of regeneration—cell division, new blood vessel growth, collagen production, stem cell activation—all of it slows to a crawl.
ENPP1 doesn’t just appear randomly. It becomes highly expressed exactly where you don’t want it—in injured oral tissues. After pulp exposure. After an extraction. Right around that fresh implant site you so carefully prepared.
So while you’re doing everything right surgically, ENPP1 may be quietly transforming a pro-healing environment into a metabolically suppressed one.
A silent saboteur, working beneath the surface.
Now that you know it’s there… the real question is: what can we do about it?
The Moment Healing Breaks: A Step-by-Step Betrayal
Picture this. A patient sits in your chair with deep caries approaching the pulp. Or perhaps you’ve just completed a periodontal flap, and everything looks textbook perfect. You’ve done your job. Now, you trust the body to do its job.
But inside that wound, invisible and silent, a betrayal is about to unfold.
Let me walk you through exactly how ENPP1 hijacks the healing process, step by step. Because understanding this cascade is the first step to stopping it.
Act One: The Injury
Tissue is damaged. Maybe from decay. Maybe from your surgical instruments. Either way, cells rupture. And as they die, they scream for help, by flooding the area with ATP. This is nature’s emergency broadcast system. It means: “Heal here. Now.”
Act Two: The Saboteur Arrives
Enter ENPP1. The enzyme doesn’t warn. It doesn’t negotiate. It simply goes to work, grabbing every ATP molecule it can find and converting it into AMP.
At first glance? Just chemistry. No big deal.
But here’s where the story turns dark.
Act Three: The Domino Effect
That newly formed AMP doesn’t just sit there. It signals neighboring cells—odontoblast-like cells, fibroblasts, the very cells you need for repair—to release two specific substances: adenine and purine nucleosides.
Innocent names. Devastating consequences.
Because those molecules do one thing exceptionally well: they shut down pyrimidine biosynthesis.
Act Four: The Collapse
Pyrimidines are the building blocks of DNA. No pyrimidines? No DNA replication. No DNA replication? No new cells. No new cells? No healing.
The clinical toll is brutal:
Fibroblasts stop multiplying, so connective tissue never forms properly
Endothelial cells die off, so new blood vessels never arrive to feed the wound
Angiogenesis grinds to a halt, so oxygen and nutrients can’t reach the site
And finally, p53-mediated pathways trigger widespread apoptosis, programmed cell death
What This Means for Your Patients
In dental terms? Let me translate.
That pulp exposure you’re trying to cap? Slower healing. Poor outcomes.
That periodontal defect you carefully grafted? Regeneration fails. Scar tissue forms instead of true repair.
That extraction socket you hoped would remodel beautifully? Fibrosis. Not healing.
ENPP1 doesn’t just slow things down. It actively changes the quality of repair, replacing regeneration with scar.
And until now, you’ve had no way to stop it.
But that’s about to change.
From the Heart to Your Chair: A Cardiac Discovery Changes Regenerative Dentistry
Let me pause for a moment. You might be thinking: “This is fascinating, but I treat teeth and gums—not heart attacks.”
Fair question. Here’s the surprising answer.
The original research on ENPP1 came from cardiac injury models. Scientists were trying to understand why some hearts heal poorly after a heart attack. And what they found was this same molecular brake,” ENPP1″, quietly sabotaging regeneration.
But here’s where the story gets personal for you.
The tissues ENPP1 attacks in the heart? Fibroblasts. Endothelial cells. Inflammatory cells. Healing pathways? ATP metabolism. Pyrimidine synthesis. Cell proliferation.
Sound familiar?
Those aren’t heart cells. Those are your cells. The same ones you depend on every single day to heal pulp, periodontium, bone, and gingiva.
Let me walk you through four scenarios you’ve likely faced this week—and show you exactly where ENPP1 has been hiding in plain sight.
1. The Pulp Cap That Failed for No Good Reason
You’ve seen it. A deep caries excavation. Direct pulp cap. Beautiful protocol. And six weeks later? No dentin bridge. Worse—the tooth needs root canal therapy.
You blamed yourself. Maybe the contamination. Maybe the material.
But consider this: ENPP1-induced metabolic disruption may have silently limited stem cell proliferation in that pulp. No proliferation? No differentiation. No dentin bridge. Just necrosis waiting to happen.
2. The Periodontal Case That Never Quite Healed
You did everything right. Flap. Debridement. Graft. Membrane. The patient complied perfectly. And yet, six months later? Attachment gain was disappointing. The defect filled with scar, not bone.
ENPP1 attacks the three cell types you needed most: fibroblasts, osteoblasts, and endothelial cells. All three. Simultaneously. The result? Fibrotic repair instead of true regeneration. Reduced attachment. A clinical failure that wasn’t your fault.
3. The Implant That Took Forever to Integrate
Some implants just feel different, don’t they? Primary stability was good. The patient healed slowly. Integration took months longer than expected. Bone quality on follow-up? Suboptimal.
Osseointegration demands rapid bone remodeling and robust vascularization. ENPP1 overactivity chokes both. Delayed integration. Poor bone quality. An implant at risk—before it even sees a crown.
4. The Extraction Socket That Healed Ugly
Simple extraction. Healthy patient. And yet, the socket filled with soft, scar-like tissue instead of beautiful, ridge-forming bone. The future implant site? Compromised before you started.
ENPP1 promotes inflammation. Slows cell turnover. And worst of all, favors scar over bone. Exactly what you don’t want in an extraction site.
This isn’t theoretical. These aren’t lab-bench curiosities. These are your Monday mornings. Your failed pulp caps. Your sluggish periodontals. Your slow implants. Your ugly sockets.
ENPP1 has been there all along.
Now that you know its name… let’s talk about what you can do about it.
The Wrong Question We’ve Been Asking for Decades
Stop for a moment and think about how we practice regenerative dentistry today.
We take a surgical site—say, a periodontal defect or an extraction socket—and what do we do? We pour in growth factors. Pack it with biomaterials. Sometimes even transplant stem cells.
The underlying assumption has always been the same: healing fails because something is missing.
So we add more. More BMPs. More scaffolds. More cells. More, more, more.
And yet, cases still fail. Pulps don’t cap. Implants don’t integrate. Periodontal defects scar instead of regenerate.
Maybe—just maybe—we’ve been asking the wrong question all along.
What If the Problem Isn’t Absence, but Presence?
Here’s what the ENPP1 model taught us, and it changes everything.
What if healing fails not because something is missing—but because something is actively blocking the process?
Think of it like this. You’re trying to drive a car. The engine won’t start. So you keep adding more fuel. More air. More spark.
But the real problem? Someone left the parking brake on.
ENPP1 is that parking brake.
And no amount of growth factors will overcome a brake that’s fully engaged.
The Shift: From Adding to Removing
This is the paradigm shift I want you to walk away with today.
| Traditional Approach | ENPP1-Based Approach |
|---|---|
| Force regeneration | Remove inhibition |
| Add growth factors | Block ENPP1 activity |
| Overstimulate cells | Restore normal metabolism |
| Fight the wound | Let the body heal itself |
Which one sounds more elegant to you?
Instead of pushing tissues uphill against a molecular brake, we simply release the brake—and let the body’s own remarkable repair machinery do what it evolved to do.
This isn’t theoretical. The biology is already there, inside every patient. We just have to stop sabotaging it.
Three Ways to Release the Brake—Today and Tomorrow
So how do we actually do this? Researchers have identified three distinct strategies. Two are still on the horizon. One is surprisingly simple.
Strategy 1: ENPP1 Inhibitors or Anti-ENPP1 (Coming Soon)
Small molecule inhibitors exist right now. Flavonoid-based compounds like myricetin have already shown they can reduce cell death and improve tissue repair.
Imagine walking into your operatory five years from now and reaching for:
A post-surgical healing gel that blocks ENPP1 at the extraction site
An implant surface coating that releases inhibitor directly into the bone
An endodontic medicament that protects the pulp during vital therapy
Not science fiction. Just smart pharmacology.
Strategy 2: Monoclonal Antibodies (The Precision Strike)
For more targeted cases, we could use antibodies that bind ENPP1 directly—neutralizing it like a guided missile.
The dental applications are breathtaking:
An injectable therapy for a stubborn periodontal defect
An adjunct injection during regenerative endodontics
A local shot at the time of implant placement
No systemic side effects. No off-target issues. Just a precise removal of the brake, exactly where you need it.
Strategy 3: Pyrimidine Supplementation (The Elegant Surprise)
And now, let me share the most compelling finding of all.
Remember how ENPP1 shuts down pyrimidine biosynthesis—the very building blocks of DNA? What if we simply gave those building blocks back?
Researchers tried exactly that. With a simple, natural molecule called uridine.
The results were stunning. Uridine supplementation restored pyrimidine balance. Prevented DNA damage. Rescued healing completely.
In dental terms:
A nutritional adjunct patients could take before and after surgery
A local delivery system mixed into your bone graft material
A simple, low-cost way to support regeneration from the inside out
For decades, we’ve been forcing growth. Adding more. Pushing harder.
The ENPP1 model offers something better: remove the brake, step back, and let the body do what it already knows how to do.
That’s not just a new technique. That’s a new philosophy.
And it might just change the way you treat your next patient.
The Question You’ve Asked Yourself a Hundred Times
Haven’t you ever had a case that should have healed perfectly, but didn’t?
Clean surgery. Healthy patient. Good materials. Perfect technique. And yet, the regeneration failed. The pulp necrosed. The implant lagged. The socket filled with scar instead of bone.
You replayed every step. You couldn’t find your mistake. Because there wasn’t one.
For years, we’ve called these “unpredictable outcomes.” A polite way of saying: we don’t know why.
But what if I told you that ENPP1 just handed you the missing explanation?
The Real Reason Some Cases Fail (Hint: It’s Not Your Technique)
Let me reframe everything you just learned into one clear, clinical truth:
Healing failure isn’t always about infection, poor blood supply, or surgical error.
Sometimes, it’s metabolic.
ENPP1 creates three specific, measurable problems inside a healing wound:
Metabolic imbalance: The ATP-to-AMP shift starves cells of the energy they need to rebuild.
Loss of proliferative capacity: Fibroblasts, osteoblasts, and stem cells stop multiplying.
DNA damage: Without pyrimidines, regenerating tissues literally cannot copy their genetic code.
That’s not a technique failure. That’s biology slamming the brakes.
And once you understand that, your diagnostic perspective shifts forever. You stop asking only “What did I do wrong?” and start asking “Was the metabolic brake engaged?”
Where Do We Go From Here? The Next Decade of Dentistry
The discovery of ENPP1 isn’t just a footnote in a biochemistry journal. It’s a roadmap. Here is where this road leads.
1. Metabolic Modulation
The future dentist won’t just clean and fill. They will manage cellular metabolism. Small molecules, local delivery systems, and targeted inhibitors will become as common as local anesthetics.
2. Precision Regenerative Therapy
Imagine this: you take a small tissue sample from a chronic periodontal defect. A chairside test measures ENPP1 activity. You then customize the treatment—more inhibitor, more uridine, or both—specifically for that patient, that site, that wound.
Not one-size-fits-all. Precision healing.
3. Combination Therapies
Why choose between growth factors and ENPP1 inhibitors? The future is both.
Biomaterials to scaffold the wound
Growth factors to stimulate cells
ENPP1 inhibitors to release the brake
Three tools. One goal. Unstoppable regeneration.
4. Chairside Biological Interventions
No waiting for labs. No systemic medications. Just a syringe, a gel, or a coating applied during the procedure. Rapid. Localized. Powerful.
You place the implant. You coat it with an ENPP1 inhibitor. You close.
And for the first time, you know you’ve removed the hidden barrier to healing.
A New Frontier: Removing the Invisible Hand Brake
Let me leave you with this.
For decades, regenerative dentistry has been a story of addition. Add growth factors. Add cells. Add scaffolds. Push harder.
ENPP1 tells us a different story. A better one.
Healing is not always limited by lack of stimulation.
Sometimes, it is limited by active biological suppression.
Think about the power of that sentence.
It means that inside every wound that failed to heal, there wasn’t a deficit of healing signals. There was a blockade.
And now, for the first time, we know how to remove it.
The Gateway to True Regeneration
ENPP1 is not just another protein. It’s not a footnote. It’s not a lab curiosity.
It is a gateway.
A gateway to faster healing. More predictable regeneration. Biologically optimized outcomes.
For you, the clinician, it means fewer sleepless nights wondering why a good case went bad.
For your patients, it means wounds that truly heal. Pulps that regenerate. Implants that integrate. Sockets that become bone.
The brake has a name now. ENPP1.
And now that you know its name… you know exactly what to do.
Frequently Asked Questions (FAQ) About ENPP1
1. What is ENPP1 in simple terms?
ENPP1 is an enzyme found on the surface of cells that regulates how energy molecules like ATP are used outside the cell. In the context of healing, it acts like a biological “brake”, reducing the signals that normally promote tissue repair and regeneration.
2. Why is ENPP1 important in dental treatments?
ENPP1 directly affects how well oral tissues heal after procedures such as fillings, root canals, implants, or extractions. High ENPP1 activity can:
- Slow down tissue regeneration
- Reduce blood vessel formation
- Increase the risk of incomplete healing
This makes it a key factor in determining treatment success or failure.
3. Does ENPP1 affect dental implants?
Yes, potentially. Successful implant integration depends on strong bone healing and vascularization. Elevated ENPP1 activity may:
- Delay bone formation
- Reduce implant stability over time
- Contribute to early implant failure in some cases
This is why targeting ENPP1 could improve osseointegration outcomes in the future.
4. Can ENPP1 impact root canal or pulp treatments?
Absolutely. In procedures like vital pulp therapy or regenerative endodontics, healing relies on stem cell activity and dentin formation. ENPP1 may:
- Inhibit stem cell proliferation
- Reduce dentin bridge formation
- Increase the likelihood of pulp necrosis
Controlling ENPP1 could significantly improve pulp preservation strategies.
5. Are there treatments available now that target ENPP1?
Currently, ENPP1-targeted therapies are still in the research and experimental stage. However, promising approaches include:
- Small molecule inhibitors
- Monoclonal antibodies
- Metabolic support therapies مثل uridine
These may become part of clinical dentistry in the near future.
6. How could dentists use ENPP1 inhibition in practice?
In the future, dentists might apply ENPP1-targeting therapies through:
- Local gels or medicaments after surgery
- Coatings on dental implants
- Additives in bone graft materials
The goal would be to enhance natural healing rather than forcing it.
7. Does ENPP1 explain why some patients heal slower than others?
It could be one of the key reasons. Variations in ENPP1 expression or activity may lead to:
- Slower cell regeneration
- Increased inflammation
- Higher risk of fibrosis instead of true healing
This supports the idea of personalized dentistry based on molecular biology.
8. Is ENPP1 related to inflammation or infection?
Indirectly, yes. ENPP1 is activated during tissue injury and inflammation. While it does not cause infection, it can:
- Prolong inflammatory responses
- Reduce the efficiency of tissue repair
This makes it an important link between inflammation and impaired healing.
9. What is the future of ENPP1 research in dentistry?
Research is moving toward integrating ENPP1 modulation into regenerative protocols, including:
- Stem cell therapies
- Tissue engineering
- Advanced biomaterials
In the long term, controlling ENPP1 could become a standard component of advanced dental care.
Reference:
Cardiomyocytes disrupt pyrimidine biosynthesis in nonmyocytes to regulate heart repair
Shen Li, Tomohiro Yokota, Ping Wang, Johanna ten Hoeve, Feiyang Ma, Thuc M. Le, Evan R. Abt, Yonggang Zhou, Rimao Wu, Maxine Nanthavongdouangsy, Abraham Rodriguez, Yijie Wang, Yen-Ju Lin, Hayato Muranaka, Mark Sharpley, Demetrios T. Braddock, Vicky E. MacRae, Utpal Banerjee, Pei-Yu Chiou, Marcus Seldin, Dian Huang, Michael Teitell, Ilya Gertsman, Michael Jung, Steven J. Bensinger, Robert Damoiseaux, Kym Faull, Matteo Pellegrini, Aldons J. Lusis, Thomas G. Graeber, Caius G. Radu, and Arjun Deb.
Recent Articles
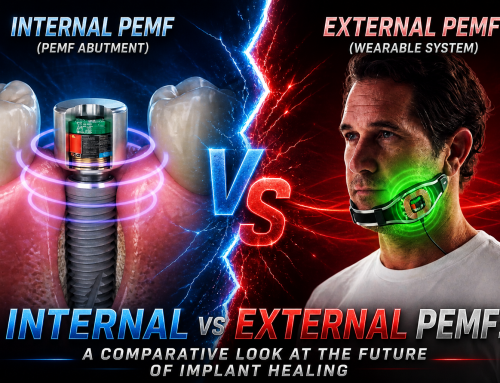
Pulsed Electromagnetic Field (PEMF) Use in Implant Dentistry
Pulsed Electromagnetic Field (PEMF) Use in Implant Dentistry Abstract and Historical Background Pulsed Electromagnetic Field (PEMF) therapy refers to the application of low-frequency electromagnetic [...]
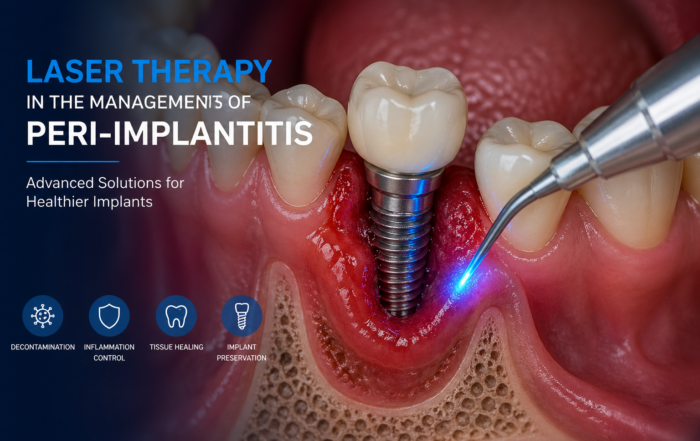
Laser Therapy in the Management of Peri-Implantitis
Laser Therapy in the Management of Peri-Implantitis Laser technology has become an increasingly valuable adjunct in the treatment of peri-implant diseases, particularly peri-implantitis. Its [...]
Magnetically Guided Dental Nanobots (CalBots) Are Real
Magnetically Guided Dental Nanobots (CalBots) Are Real The concept of nanobots in dentistry has long been associated with futuristic speculation. However, recent peer-reviewed research [...]

Peri-Implantitis Treatment & Prevention Methods
Peri-Implantitis Treatment & Prevention Methods Peri-implantitis remains one of the most significant biological complications affecting dental implants, posing a serious threat to long-term implant [...]
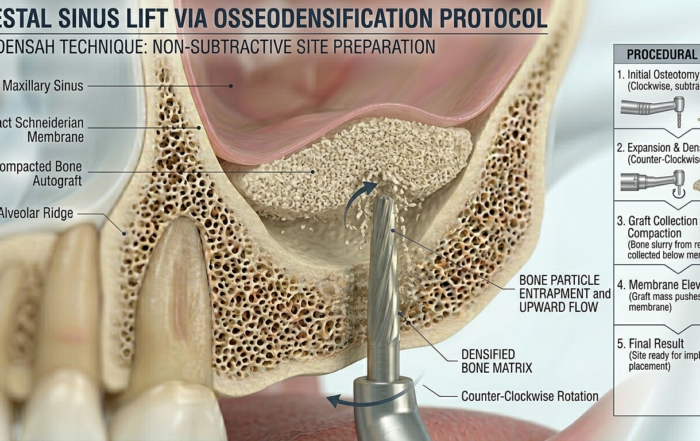
Latest Sinus Lifting Techniques in Modern Implant Dentistry
Latest Sinus Lifting Techniques in Modern Implant Dentistry A Comprehensive Clinical Review Introduction to Sinus Lifting in Implantology Sinus lifting, or maxillary sinus floor [...]

Biomechanics of the Triple Abutment & BOPiT Concept
Dental Biomechanics · Implant Science · Clinical Evidence Biomechanics of the Triple Abutment & BOPiT Concept How a saddle-shaped mathematical surface is rewriting the rules of load distribution [...]





Follow Us
{kind=link}
{kind=link}
{kind=link}