

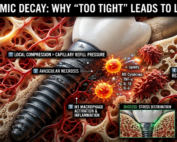
When “Perfectly Tight” Dental Implants Fail
The Hidden Role of Ischemic Bone Resorption and Osteoimmune Dysfunction
In modern dental implantology, achieving high primary stability is often considered a cornerstone of successful osseointegration. Implantologists routinely pursue strong insertion torque values, firm cortical engagement, and rigid initial fixation to minimize micromotion and improve immediate loading outcomes. Yet an increasingly recognized biological paradox challenges this conventional mechanical mindset:
Sometimes, implants that are “too tight” may ultimately loosen.
This phenomenon appears contradictory at first glance. If insufficient stability causes failure, how could excessive stability create the same outcome? The answer lies in the complex interaction between bone physiology, microvascular perfusion, and the osteoimmune response.
Biology, not mechanics alone, determines long-term implant success.
The Traditional Pursuit of Maximum Primary Stability
Primary stability refers to the mechanical engagement between an implant and surrounding bone immediately after placement. High primary stability reduces early micromotion and creates favorable conditions for secondary biologic fixation during osseointegration.
For decades, clinicians have associated higher insertion torque with superior outcomes. Surgical protocols frequently emphasize under-preparation of osteotomies, aggressive thread engagement, and dense cortical compression to maximize implant fixation.
While adequate stability remains essential, excessive compressive strain may inadvertently compromise the surrounding bone’s vascular integrity.
Bone is not an inert structural material. It is a living, perfused tissue highly dependent on microcirculation for survival.
When implant insertion forces exceed the physiologic tolerance of the peri-implant capillary network, ischemic injury may begin almost immediately.

The Ischemic Trigger: When Compression Becomes Pathologic
The peri-implant interface contains a delicate intraosseous microvascular system responsible for delivering oxygen, nutrients, immune mediators, and osteogenic cells to adjacent bone.
Excessive compression during implant insertion can occlude these microvessels, especially in dense cortical bone or when oversized implants are placed into underprepared osteotomies.
This localized vascular compromise initiates a micro-zone of ischemic injury directly adjacent to the implant surface.
At the cellular level, osteocytes trapped within compressed bone lose perfusion and begin to undergo apoptosis or necrosis. The affected bone may initially appear mechanically stable, but biologically it has already entered a degenerative cascade.
This is one of the most overlooked concepts in implant dentistry: mechanical rigidity does not necessarily equal biologic compatibility.
An implant can feel exceptionally stable on the day of placement while simultaneously initiating tissue injury that undermines long-term osseointegration.

Osteocyte Death and the Release of DAMPs
As ischemic bone injury progresses, dying osteocytes release intracellular molecules known as Damage-Associated Molecular Patterns (DAMPs).
These molecules function as alarm signals to the innate immune system. Resident macrophages and immune surveillance cells detect DAMPs through pattern-recognition receptors, triggering an inflammatory response designed to remove damaged tissue.
Initially, this response is protective and necessary.
The problem emerges when excessive compression produces a large volume of ischemic bone that requires substantial remodeling before healthy osseointegration can occur.
The immune system interprets necrotic peri-implant bone not as stable fixation, but as damaged tissue requiring debridement.
The M1 Macrophage Response and Inflammatory Bone Resorption
Following ischemic injury, macrophages polarize toward a pro-inflammatory M1 phenotype.
M1 macrophages release inflammatory cytokines including:
- Tumor Necrosis Factor-alpha (TNF-α)
- Interleukin-1 beta (IL-1β)
- Interleukin-6 (IL-6)
These mediators stimulate osteoclastogenesis through alteration of the RANKL/OPG signaling balance.
Under physiologic conditions, osteoblasts and stromal cells regulate bone remodeling through equilibrium between:
- RANKL (Receptor Activator of Nuclear Factor Kappa-B Ligand)
- OPG (Osteoprotegerin)
When inflammatory cytokines dominate, RANKL expression increases while OPG decreases, producing aggressive osteoclast recruitment and accelerated bone resorption.
The body is essentially attempting to remove necrotic tissue created by ischemic compression.
Ironically, the very insertion torque intended to maximize stability may trigger the biologic mechanisms that reduce it.
Understanding the “Dental Dip” in Implant Stability
Most implantologists are familiar with the transient reduction in implant stability occurring between approximately weeks 2 and 6 after placement.
This phenomenon, often called the “dental dip,” reflects the transition between primary mechanical fixation and secondary biologic stability.
During this period:
- Necrotic compressed bone is resorbed
- Osteoclast activity increases
- Initial mechanical engagement weakens
- New woven bone formation begins
Eventually, healthy osseointegration restores stability through secondary bone formation.
In successful cases, the inflammatory phase transitions into regenerative healing characterized by M2 macrophage polarization, angiogenesis, and osteoblastic activity.
However, if compressive injury is excessive, or if implant biomechanics continue generating pathologic stress concentrations, the inflammatory phase may persist far longer than intended.
Chronic Inflammation and Aseptic Implant Loosening
The risk becomes even greater in orthopedic reconstructions and heavily loaded implant systems, but the principles remain highly relevant to dental implantology.
When implant geometry produces excessive point loading, stress shielding, or abnormal rigidity, the peri-implant environment may remain chronically inflammatory.
Instead of transitioning from an M1 inflammatory phenotype toward a regenerative M2 healing phenotype, macrophages continue promoting osteoclastic activity and bone destruction.
This creates a self-perpetuating osteoimmune loop:
- Mechanical overload causes microdamage
- Microdamage triggers inflammation
- Inflammation stimulates osteoclasts
- Bone resorption weakens support
- Altered load distribution increases further stress
Over time, the result may become aseptic implant loosening.
Notably, this process can occur even in the absence of bacterial infection.
This distinction is critical because clinicians frequently attribute marginal bone loss solely to peri-implantitis or occlusal overload, while underestimating the role of insertion-related ischemic trauma and chronic osteoimmune dysregulation.
Why Implant Design Must Respect Perfusion Biology
Modern implant innovation has heavily emphasized surface treatments, roughness optimization, and thread aggressiveness.
While these factors remain important, the future of implant design increasingly requires a more biologically integrated engineering philosophy.
True primary stability is not simply about forcing an implant tightly into bone.
It is about achieving physiologic load distribution that preserves vascular perfusion while minimizing destructive strain concentrations.
This requires careful consideration of:
- Implant geometry
- Thread design
- Elastic modulus compatibility
- Load transfer dynamics
- Stress distribution patterns
- Cortical compression thresholds
Excessively rigid systems may create stress shielding, where surrounding bone experiences insufficient physiologic stimulation and undergoes resorption according to Wolff’s Law.
Conversely, excessive point compression may induce ischemic necrosis and inflammatory remodeling.
The optimal implant is therefore not the tightest implant, but the most biologically compatible implant.
Surgical Implications for Dental Implantologists
For clinicians, these concepts have important practical implications during treatment planning and surgical execution.
Strategies that may help reduce ischemic peri-implant injury include:
Respecting Bone Density Variations
Dense cortical bone requires different osteotomy preparation compared with softer cancellous bone. Excessive under-preparation in D1 bone may dramatically increase compressive strain.
Avoiding Excessive Insertion Torque
Very high insertion torque values are not universally beneficial. Beyond a certain threshold, increasing torque may contribute more to vascular compromise than to meaningful stability gains.
Optimizing Osteotomy Preparation
Precise osteotomy protocols should balance stability with physiologic strain distribution rather than maximizing compression alone.
Considering Implant Elasticity and Geometry
Implant macrodesign influences load transfer behavior and peri-implant stress concentrations. More biomimetic designs may better preserve surrounding bone physiology.
Monitoring Early Stability Changes
Understanding the biologic basis of the “dental dip” allows clinicians to interpret transient stability reductions more accurately during early healing phases.
The Future of Implantology: Osteoimmunology and Biomechanical Harmony
The future of implant dentistry will likely move beyond purely mechanical concepts toward an integrated osteoimmunologic model.
Osseointegration is not simply a structural event. It is an immune-mediated biologic negotiation between implant surfaces, bone cells, vascular systems, and inflammatory signaling pathways.
Successful implants do not merely resist motion mechanically.
They cooperate biologically with surrounding tissues.
This shift in perspective has profound implications for implant design, surgical protocols, biomaterials research, and long-term patient outcomes.
As implantology advances, the profession must increasingly recognize that aggressive mechanical fixation alone cannot guarantee success.
Perfusion biology matters.
Microvascular preservation matters.
Macrophage polarization matters.
And ultimately, biology always gets the final word.
Conclusion
The concept that “too-tight” implants may fail through ischemic bone injury challenges many traditional assumptions in dental implantology. Excessive compression can compromise peri-implant vascular perfusion, trigger osteocyte death, activate inflammatory osteoimmune pathways, and initiate osteoclastic bone resorption.
While adequate primary stability remains essential, the goal should not be brute-force fixation. Instead, clinicians and implant manufacturers must pursue physiologic load distribution that preserves vascular integrity and supports healthy biologic healing.
The most successful implants are not necessarily the tightest implants.
They are the implants that best respect the biology of bone.
Here are 10 SEO-optimized FAQs with scientifically grounded answers and reference citations suitable for a professional dental implantology article.
Frequently Asked Questions (FAQs)
1. Can dental implants fail because they are inserted too tightly?
Yes. Excessive insertion torque and over-compression of peri-implant bone can impair microvascular perfusion, leading to ischemic bone injury and subsequent bone resorption. Although high primary stability is important, excessive compressive strain may create necrotic bone zones that require remodeling before osseointegration can occur.
References:
- Frost HM. Bone “mass” and the “mechanostat”: a proposal. Anatomical Record. 1987.
- Trisi P, et al. Implant micromotion is related to peak insertion torque and bone density. Clinical Oral Implants Research. 2009.
- Bashutski JD, Wang HL. Common implant esthetic complications. Implant Dentistry. 2007.
2. What is the “dental dip” in implant stability?
The “dental dip” refers to the temporary reduction in implant stability that commonly occurs between weeks 2 and 6 after implant placement. During this phase, necrotic compressed bone is resorbed by osteoclasts before secondary biologic fixation develops through new bone formation.
References:
- Raghavendra S, et al. Early wound healing around endosseous implants. Journal of Periodontology. 2005.
- Berglundh T, et al. The soft tissue barrier at implants and teeth. Clinical Oral Implants Research. 1991.
3. Why does excessive implant compression cause bone resorption?
Excessive compression can obstruct intraosseous blood vessels, causing localized ischemia. Dying osteocytes release inflammatory signals known as Damage-Associated Molecular Patterns (DAMPs), which activate macrophages and promote osteoclast-mediated bone resorption.
References:
- Anderson JM, Rodriguez A, Chang DT. Foreign body reaction to biomaterials. Seminars in Immunology. 2008.
- Takayanagi H. Osteoimmunology and the effects of the immune system on bone. Nature Reviews Rheumatology. 2009.
4. What role do macrophages play in implant osseointegration?
Macrophages regulate the inflammatory and healing response around implants. M1 macrophages promote inflammation and tissue breakdown, while M2 macrophages support angiogenesis, tissue repair, and bone regeneration. Successful osseointegration requires transition from an M1-dominant state to an M2 healing environment.
References:
- Brown BN, et al. Macrophage polarization in tissue engineering. Acta Biomaterialia. 2012.
- Franz S, et al. Immune responses to implants. Biomaterials. 2011.
5. Is higher insertion torque always better for implant success?
No. While inadequate stability increases failure risk, excessively high insertion torque may damage surrounding bone and impair healing. Modern implantology increasingly emphasizes physiologic load distribution rather than brute-force mechanical fixation.
References:
- Ottoni JM, et al. Correlation between placement torque and survival of single-tooth implants. International Journal of Oral & Maxillofacial Implants. 2005.
- Trisi P, et al. Bone-implant contact and bone quality evaluation. Clinical Oral Implants Research. 1999.
6. What is stress shielding in dental implants?
Stress shielding occurs when an implant is excessively rigid and absorbs too much functional load, reducing physiologic stress transfer to surrounding bone. According to Wolff’s Law, insufficient mechanical stimulation can lead to bone remodeling and resorption.
References:
- Huiskes R, et al. Effects of mechanical forces on maintenance and adaptation of form in trabecular bone. Nature. 2000.
- Frost HM. Wolff’s Law and bone’s structural adaptations to mechanical usage. Orthopedic Clinics of North America. 1987.
7. How does implant geometry influence peri-implant bone health?
Implant macrodesign, thread geometry, and elasticity influence how forces are distributed within surrounding bone. Poor load distribution may create stress concentrations and microdamage that perpetuate inflammation and osteoclastic activity.
References:
- Misch CE. Contemporary Implant Dentistry. 3rd Edition. Mosby Elsevier.
- Geng JP, et al. Application of finite element analysis in implant dentistry. Journal of Prosthetic Dentistry. 2001.
8. Can implant loosening occur without bacterial infection?
Yes. Aseptic loosening can occur when chronic mechanical overload and persistent inflammatory signaling drive osteoclastic bone resorption in the absence of infection. This phenomenon is well documented in orthopedic implantology and has parallels in dental implantology.
References:
- Purdue PE, et al. The central role of wear debris in periprosthetic osteolysis. HSS Journal. 2006.
- Goodman SB, et al. Cellular profile and cytokine production at prosthetic interfaces. Clinical Orthopaedics and Related Research. 1998.
9. Why is vascular perfusion important during osseointegration?
Bone healing depends on adequate blood supply for oxygen delivery, nutrient transport, angiogenesis, and recruitment of osteogenic cells. Compromised microcirculation may delay healing and increase the risk of inflammatory bone loss.
References:
- Davies JE. Understanding peri-implant endosseous healing. Journal of Dental Education. 2003.
- Albrektsson T, et al. The long-term efficacy of currently used dental implants. European Journal of Oral Sciences. 1981.
10. What is the future direction of implantology research?
Future implantology research is increasingly focused on osteoimmunology, biomimetic implant design, controlled load transfer, and preservation of peri-implant vascular biology. The goal is to create implants that are mechanically stable while remaining biologically compatible with bone physiology.
References:
- Chen Z, Klein T, Murray RZ, Crawford R, Chang J, Wu C, Xiao Y. Osteoimmunomodulation for the development of advanced bone biomaterials. Materials Today. 2016.
- Shah FA, et al. Osteoimmunomodulation and osseointegration. Clinical Implant Dentistry and Related Research. 2019.
Recent Articles





































In modern dental implantology, achieving high primary stability is often considered a cornerstone of successful osseointegration. Implantologists routinely pursue strong insertion torque values, firm cortical engagement, and rigid initial fixation to minimize micromotion and improve immediate loading outcomes. Yet an increasingly recognized biological paradox challenges this conventional mechanical mindset:
Sometimes, implants that are “too tight” may ultimately loosen.
This phenomenon appears contradictory at first glance. If insufficient stability causes failure, how could excessive stability create the same outcome? The answer lies in the complex interaction between bone physiology, microvascular perfusion, and the osteoimmune response.
Biology, not mechanics alone, determines long-term implant success.
The Traditional Pursuit of Maximum Primary Stability
Primary stability refers to the mechanical engagement between an implant and surrounding bone immediately after placement. High primary stability reduces early micromotion and creates favorable conditions for secondary biologic fixation during osseointegration.
For decades, clinicians have associated higher insertion torque with superior outcomes. Surgical protocols frequently emphasize under-preparation of osteotomies, aggressive thread engagement, and dense cortical compression to maximize implant fixation.
While adequate stability remains essential, excessive compressive strain may inadvertently compromise the surrounding bone’s vascular integrity.
Bone is not an inert structural material. It is a living, perfused tissue highly dependent on microcirculation for survival.
When implant insertion forces exceed the physiologic tolerance of the peri-implant capillary network, ischemic injury may begin almost immediately.
The Ischemic Trigger: When Compression Becomes Pathologic
The peri-implant interface contains a delicate intraosseous microvascular system responsible for delivering oxygen, nutrients, immune mediators, and osteogenic cells to adjacent bone.
Excessive compression during implant insertion can occlude these microvessels, especially in dense cortical bone or when oversized implants are placed into underprepared osteotomies.
This localized vascular compromise initiates a micro-zone of ischemic injury directly adjacent to the implant surface.
At the cellular level, osteocytes trapped within compressed bone lose perfusion and begin to undergo apoptosis or necrosis. The affected bone may initially appear mechanically stable, but biologically it has already entered a degenerative cascade.
This is one of the most overlooked concepts in implant dentistry: mechanical rigidity does not necessarily equal biologic compatibility.
An implant can feel exceptionally stable on the day of placement while simultaneously initiating tissue injury that undermines long-term osseointegration.
Osteocyte Death and the Release of DAMPs
As ischemic bone injury progresses, dying osteocytes release intracellular molecules known as Damage-Associated Molecular Patterns (DAMPs).
These molecules function as alarm signals to the innate immune system. Resident macrophages and immune surveillance cells detect DAMPs through pattern-recognition receptors, triggering an inflammatory response designed to remove damaged tissue.
Initially, this response is protective and necessary.
The problem emerges when excessive compression produces a large volume of ischemic bone that requires substantial remodeling before healthy osseointegration can occur.
The immune system interprets necrotic peri-implant bone not as stable fixation, but as damaged tissue requiring debridement.
The M1 Macrophage Response and Inflammatory Bone Resorption
Following ischemic injury, macrophages polarize toward a pro-inflammatory M1 phenotype.
M1 macrophages release inflammatory cytokines including:
- Tumor Necrosis Factor-alpha (TNF-α)
- Interleukin-1 beta (IL-1β)
- Interleukin-6 (IL-6)
These mediators stimulate osteoclastogenesis through alteration of the RANKL/OPG signaling balance.
Under physiologic conditions, osteoblasts and stromal cells regulate bone remodeling through equilibrium between:
- RANKL (Receptor Activator of Nuclear Factor Kappa-B Ligand)
- OPG (Osteoprotegerin)
When inflammatory cytokines dominate, RANKL expression increases while OPG decreases, producing aggressive osteoclast recruitment and accelerated bone resorption.
The body is essentially attempting to remove necrotic tissue created by ischemic compression.
Ironically, the very insertion torque intended to maximize stability may trigger the biologic mechanisms that reduce it.
Understanding the “Dental Dip” in Implant Stability
Most implantologists are familiar with the transient reduction in implant stability occurring between approximately weeks 2 and 6 after placement.
This phenomenon, often called the “dental dip,” reflects the transition between primary mechanical fixation and secondary biologic stability.
During this period:
- Necrotic compressed bone is resorbed
- Osteoclast activity increases
- Initial mechanical engagement weakens
- New woven bone formation begins
Eventually, healthy osseointegration restores stability through secondary bone formation.
In successful cases, the inflammatory phase transitions into regenerative healing characterized by M2 macrophage polarization, angiogenesis, and osteoblastic activity.
However, if compressive injury is excessive, or if implant biomechanics continue generating pathologic stress concentrations, the inflammatory phase may persist far longer than intended.
Chronic Inflammation and Aseptic Implant Loosening
The risk becomes even greater in orthopedic reconstructions and heavily loaded implant systems, but the principles remain highly relevant to dental implantology.
When implant geometry produces excessive point loading, stress shielding, or abnormal rigidity, the peri-implant environment may remain chronically inflammatory.
Instead of transitioning from an M1 inflammatory phenotype toward a regenerative M2 healing phenotype, macrophages continue promoting osteoclastic activity and bone destruction.
This creates a self-perpetuating osteoimmune loop:
- Mechanical overload causes microdamage
- Microdamage triggers inflammation
- Inflammation stimulates osteoclasts
- Bone resorption weakens support
- Altered load distribution increases further stress
Over time, the result may become aseptic implant loosening.
Notably, this process can occur even in the absence of bacterial infection.
This distinction is critical because clinicians frequently attribute marginal bone loss solely to peri-implantitis or occlusal overload, while underestimating the role of insertion-related ischemic trauma and chronic osteoimmune dysregulation.
Why Implant Design Must Respect Perfusion Biology
Modern implant innovation has heavily emphasized surface treatments, roughness optimization, and thread aggressiveness.
While these factors remain important, the future of implant design increasingly requires a more biologically integrated engineering philosophy.
True primary stability is not simply about forcing an implant tightly into bone.
It is about achieving physiologic load distribution that preserves vascular perfusion while minimizing destructive strain concentrations.
This requires careful consideration of:
- Implant geometry
- Thread design
- Elastic modulus compatibility
- Load transfer dynamics
- Stress distribution patterns
- Cortical compression thresholds
Excessively rigid systems may create stress shielding, where surrounding bone experiences insufficient physiologic stimulation and undergoes resorption according to Wolff’s Law.
Conversely, excessive point compression may induce ischemic necrosis and inflammatory remodeling.
The optimal implant is therefore not the tightest implant, but the most biologically compatible implant.
Surgical Implications for Dental Implantologists
For clinicians, these concepts have important practical implications during treatment planning and surgical execution.
Strategies that may help reduce ischemic peri-implant injury include:
Respecting Bone Density Variations
Dense cortical bone requires different osteotomy preparation compared with softer cancellous bone. Excessive under-preparation in D1 bone may dramatically increase compressive strain.
Avoiding Excessive Insertion Torque
Very high insertion torque values are not universally beneficial. Beyond a certain threshold, increasing torque may contribute more to vascular compromise than to meaningful stability gains.
Optimizing Osteotomy Preparation
Precise osteotomy protocols should balance stability with physiologic strain distribution rather than maximizing compression alone.
Considering Implant Elasticity and Geometry
Implant macrodesign influences load transfer behavior and peri-implant stress concentrations. More biomimetic designs may better preserve surrounding bone physiology.
Monitoring Early Stability Changes
Understanding the biologic basis of the “dental dip” allows clinicians to interpret transient stability reductions more accurately during early healing phases.
The Future of Implantology: Osteoimmunology and Biomechanical Harmony
The future of implant dentistry will likely move beyond purely mechanical concepts toward an integrated osteoimmunologic model.
Osseointegration is not simply a structural event. It is an immune-mediated biologic negotiation between implant surfaces, bone cells, vascular systems, and inflammatory signaling pathways.
Successful implants do not merely resist motion mechanically.
They cooperate biologically with surrounding tissues.
This shift in perspective has profound implications for implant design, surgical protocols, biomaterials research, and long-term patient outcomes.
As implantology advances, the profession must increasingly recognize that aggressive mechanical fixation alone cannot guarantee success.
Perfusion biology matters.
Microvascular preservation matters.
Macrophage polarization matters.
And ultimately, biology always gets the final word.
Conclusion
The concept that “too-tight” implants may fail through ischemic bone injury challenges many traditional assumptions in dental implantology. Excessive compression can compromise peri-implant vascular perfusion, trigger osteocyte death, activate inflammatory osteoimmune pathways, and initiate osteoclastic bone resorption.
While adequate primary stability remains essential, the goal should not be brute-force fixation. Instead, clinicians and implant manufacturers must pursue physiologic load distribution that preserves vascular integrity and supports healthy biologic healing.
The most successful implants are not necessarily the tightest implants.
They are the implants that best respect the biology of bone.
Here are 10 SEO-optimized FAQs with scientifically grounded answers and reference citations suitable for a professional dental implantology article.
Frequently Asked Questions (FAQs)
1. Can dental implants fail because they are inserted too tightly?
Yes. Excessive insertion torque and over-compression of peri-implant bone can impair microvascular perfusion, leading to ischemic bone injury and subsequent bone resorption. Although high primary stability is important, excessive compressive strain may create necrotic bone zones that require remodeling before osseointegration can occur.
References:
- Frost HM. Bone “mass” and the “mechanostat”: a proposal. Anatomical Record. 1987.
- Trisi P, et al. Implant micromotion is related to peak insertion torque and bone density. Clinical Oral Implants Research. 2009.
- Bashutski JD, Wang HL. Common implant esthetic complications. Implant Dentistry. 2007.
2. What is the “dental dip” in implant stability?
The “dental dip” refers to the temporary reduction in implant stability that commonly occurs between weeks 2 and 6 after implant placement. During this phase, necrotic compressed bone is resorbed by osteoclasts before secondary biologic fixation develops through new bone formation.
References:
- Raghavendra S, et al. Early wound healing around endosseous implants. Journal of Periodontology. 2005.
- Berglundh T, et al. The soft tissue barrier at implants and teeth. Clinical Oral Implants Research. 1991.
3. Why does excessive implant compression cause bone resorption?
Excessive compression can obstruct intraosseous blood vessels, causing localized ischemia. Dying osteocytes release inflammatory signals known as Damage-Associated Molecular Patterns (DAMPs), which activate macrophages and promote osteoclast-mediated bone resorption.
References:
- Anderson JM, Rodriguez A, Chang DT. Foreign body reaction to biomaterials. Seminars in Immunology. 2008.
- Takayanagi H. Osteoimmunology and the effects of the immune system on bone. Nature Reviews Rheumatology. 2009.
4. What role do macrophages play in implant osseointegration?
Macrophages regulate the inflammatory and healing response around implants. M1 macrophages promote inflammation and tissue breakdown, while M2 macrophages support angiogenesis, tissue repair, and bone regeneration. Successful osseointegration requires transition from an M1-dominant state to an M2 healing environment.
References:
- Brown BN, et al. Macrophage polarization in tissue engineering. Acta Biomaterialia. 2012.
- Franz S, et al. Immune responses to implants. Biomaterials. 2011.
5. Is higher insertion torque always better for implant success?
No. While inadequate stability increases failure risk, excessively high insertion torque may damage surrounding bone and impair healing. Modern implantology increasingly emphasizes physiologic load distribution rather than brute-force mechanical fixation.
References:
- Ottoni JM, et al. Correlation between placement torque and survival of single-tooth implants. International Journal of Oral & Maxillofacial Implants. 2005.
- Trisi P, et al. Bone-implant contact and bone quality evaluation. Clinical Oral Implants Research. 1999.
6. What is stress shielding in dental implants?
Stress shielding occurs when an implant is excessively rigid and absorbs too much functional load, reducing physiologic stress transfer to surrounding bone. According to Wolff’s Law, insufficient mechanical stimulation can lead to bone remodeling and resorption.
References:
- Huiskes R, et al. Effects of mechanical forces on maintenance and adaptation of form in trabecular bone. Nature. 2000.
- Frost HM. Wolff’s Law and bone’s structural adaptations to mechanical usage. Orthopedic Clinics of North America. 1987.
7. How does implant geometry influence peri-implant bone health?
Implant macrodesign, thread geometry, and elasticity influence how forces are distributed within surrounding bone. Poor load distribution may create stress concentrations and microdamage that perpetuate inflammation and osteoclastic activity.
References:
- Misch CE. Contemporary Implant Dentistry. 3rd Edition. Mosby Elsevier.
- Geng JP, et al. Application of finite element analysis in implant dentistry. Journal of Prosthetic Dentistry. 2001.
8. Can implant loosening occur without bacterial infection?
Yes. Aseptic loosening can occur when chronic mechanical overload and persistent inflammatory signaling drive osteoclastic bone resorption in the absence of infection. This phenomenon is well documented in orthopedic implantology and has parallels in dental implantology.
References:
- Purdue PE, et al. The central role of wear debris in periprosthetic osteolysis. HSS Journal. 2006.
- Goodman SB, et al. Cellular profile and cytokine production at prosthetic interfaces. Clinical Orthopaedics and Related Research. 1998.
9. Why is vascular perfusion important during osseointegration?
Bone healing depends on adequate blood supply for oxygen delivery, nutrient transport, angiogenesis, and recruitment of osteogenic cells. Compromised microcirculation may delay healing and increase the risk of inflammatory bone loss.
References:
- Davies JE. Understanding peri-implant endosseous healing. Journal of Dental Education. 2003.
- Albrektsson T, et al. The long-term efficacy of currently used dental implants. European Journal of Oral Sciences. 1981.
10. What is the future direction of implantology research?
Future implantology research is increasingly focused on osteoimmunology, biomimetic implant design, controlled load transfer, and preservation of peri-implant vascular biology. The goal is to create implants that are mechanically stable while remaining biologically compatible with bone physiology.
References:
- Chen Z, Klein T, Murray RZ, Crawford R, Chang J, Wu C, Xiao Y. Osteoimmunomodulation for the development of advanced bone biomaterials. Materials Today. 2016.
- Shah FA, et al. Osteoimmunomodulation and osseointegration. Clinical Implant Dentistry and Related Research. 2019.
Recent Articles

The Bicuspidization Protocol: Engineering Meets Survival
The Bicuspidization Protocol: Engineering Meets Survival Modern restorative dentistry is no longer limited to extraction and replacement. In the era of conservative and biologically [...]
Pulsed Electromagnetic Field (PEMF) Use in Implant Dentistry
Pulsed Electromagnetic Field (PEMF) Use in Implant Dentistry Abstract and Historical Background Pulsed Electromagnetic Field (PEMF) therapy refers to the application of low-frequency electromagnetic [...]
Laser Therapy in the Management of Peri-Implantitis
Laser Therapy in the Management of Peri-Implantitis Laser technology has become an increasingly valuable adjunct in the treatment of peri-implant diseases, particularly peri-implantitis. Its [...]
Magnetically Guided Dental Nanobots (CalBots) Are Real
Magnetically Guided Dental Nanobots (CalBots) Are Real The concept of nanobots in dentistry has long been associated with futuristic speculation. However, recent peer-reviewed research [...]

Peri-Implantitis Treatment & Prevention Methods
Peri-Implantitis Treatment & Prevention Methods Peri-implantitis remains one of the most significant biological complications affecting dental implants, posing a serious threat to long-term implant [...]
Latest Sinus Lifting Techniques in Modern Implant Dentistry
Latest Sinus Lifting Techniques in Modern Implant Dentistry A Comprehensive Clinical Review Introduction to Sinus Lifting in Implantology Sinus lifting, or maxillary sinus floor [...]

{kind=link}
{kind=link}
{kind=link}