
 Use in Implant Dentistry-8ad8-a97a79c1d393")
Pulsed Electromagnetic Field (PEMF) Use in Implant Dentistry
Abstract and Historical Background
Pulsed Electromagnetic Field (PEMF) therapy refers to the application of low-frequency electromagnetic waves delivered in controlled pulses to stimulate biological tissues. Originally developed in the mid-20th century, PEMF gained medical acceptance after its successful use in enhancing bone healing and treating non-union fractures. Regulatory approval in orthopedic medicine, “particularly for delayed fracture healing”, established PEMF as a credible adjunctive therapy grounded in biophysical principles.
The transition of PEMF into dentistry began as clinicians and researchers explored its potential to accelerate osseointegration and improve peri-implant healing. Early experimental studies in the late 1990s and early 2000s demonstrated that electromagnetic stimulation could influence osteoblastic activity and bone remodeling, prompting interest in its application around dental implants. Over time, this evolved into the development of localized delivery systems designed to target peri-implant tissues during the critical healing phase.
Mechanism of Action
The biological effects of PEMF are mediated through complex cellular and molecular pathways. At the cellular level, PEMF influences transmembrane ion exchange, particularly calcium ion channels, which play a crucial role in signal transduction and cellular metabolism.
Key mechanisms include:
- Stimulation of Osteoblast Activity: PEMF enhances proliferation and differentiation of osteoblasts, increasing the production of bone matrix proteins such as collagen type I.
- Upregulation of Growth Factors: Exposure to electromagnetic fields promotes the expression of bone morphogenetic proteins (BMPs), vascular endothelial growth factor (VEGF), and transforming growth factor-beta (TGF-β).
- Enhanced Angiogenesis: Improved microvascular formation supports nutrient delivery and accelerates healing.
- Anti-inflammatory Effects: PEMF has been shown to modulate inflammatory cytokines, reducing levels of TNF-α and IL-1β during early healing.
- Improved Cellular Energy Metabolism: Increased ATP production contributes to faster tissue regeneration.
These mechanisms collectively contribute to enhanced bone formation and remodeling, particularly during the early stages of implant healing.
Effect of PEMF on Peri-Implant Tissues
The peri-implant environment consists of both hard and soft tissues that are critical for long-term implant success. PEMF appears to exert beneficial effects on both components:
1. Bone Tissue (Osseointegration)
Clinical and preclinical studies suggest that PEMF can improve early implant stability, typically measured using resonance frequency analysis (RFA) and implant stability quotient (ISQ) values. Increased bone-to-implant contact (BIC) has also been observed in animal models, indicating enhanced osseointegration.
The primary benefit appears during the early healing phase (first 2–8 weeks), where accelerated bone formation may reduce the risk of early implant failure.
2. Soft Tissue Healing
PEMF may enhance fibroblast proliferation and collagen synthesis, contributing to improved soft tissue sealing around implants. This biological seal is essential in preventing bacterial infiltration and peri-implant inflammation.
3. Inflammatory Modulation
Reduced inflammatory markers in peri-implant crevicular fluid have been reported, suggesting a more controlled healing response. This may be particularly beneficial in patients with compromised healing capacity.
Side Effects and Safety Considerations
PEMF therapy is generally considered safe when used within established parameters. However, several considerations should be acknowledged:
- Minimal Adverse Effects: Most studies report no significant side effects when PEMF is applied at therapeutic levels.
- Contraindications: Patients with pacemakers or other electronic implants may be at risk of electromagnetic interference.
- Thermal Effects: Although rare, improper calibration may lead to mild localized heating.
- Long-Term Data Limitations: There is limited evidence regarding prolonged or repeated exposure in dental applications.
Overall, PEMF demonstrates a favorable safety profile, but cautious patient selection remains essential.
Pros and Cons of Existing Studies in Implant Dentistry
Advantages of Current Evidence
- Presence of Randomized Controlled Trials (RCTs): Some clinical trials provide structured comparisons with control groups.
- Consistent Early-Phase Benefits: Multiple studies report improved implant stability during early healing.
- Biological Plausibility: Strong mechanistic support from in vitro and animal studies.
- Reproducibility in Preclinical Models: Consistent findings across different experimental setups.
Limitations of Current Evidence
- Small Sample Sizes: The only clinical study I found involved limited patient numbers (19 patients), reducing statistical power.
- Short Follow-Up Periods: The study focused on early healing without long-term outcomes.
- Use of Surrogate Endpoints: Reliance on ISQ values rather than implant survival rates.
- Potential Bias: The study is industry-supported, raising concerns about neutrality and conflicts of interest.
- Lack of Standardization: Variability in frequency, intensity, and duration of PEMF application.
These limitations highlight the need for large-scale, independent, multi-center trials to validate current findings.
Is It Wise to Use a Battery Inside an Abutment for PEMF Delivery?
The concept of integrating a power source within a healing abutment introduces both innovation and complexity. From an engineering and clinical perspective, several factors must be considered:
- Advantages:
- Localized delivery directly at the implant site
- Continuous stimulation without patient compliance dependency
- Elimination of external devices
- Concerns:
- Battery reliability and lifespan
- Risk of device failure within the oral environment
- Sterilization and biocompatibility challenges
- Increased cost compared to conventional abutments
- Lack of long-term safety data for embedded electronics
While the concept is technologically appealing, its routine clinical adoption requires further validation, particularly regarding durability and safety.
Properties of the Built-in PEMF
Built-in PEMF systems are engineered as smart healing components that integrate directly with the implant interface, allowing electromagnetic stimulation to be delivered precisely where osseointegration occurs. This localized delivery enables continuous, low-intensity field exposure throughout the critical early healing phase, without relying on patient compliance. The therapeutic concept is based on maintaining a stable electromagnetic microenvironment that supports osteoblastic activity, angiogenesis, and modulation of early inflammatory responses. Because the energy source and coil are embedded within the abutment structure, the system achieves high spatial accuracy—typically within a few millimeters of the peri-implant bone—something external devices struggle to replicate.
However, these systems operate with predefined electromagnetic parameters, meaning clinicians have limited ability to adjust frequency, intensity, or duty cycle based on individual cases. While this standardization ensures consistency, it reduces flexibility in tailoring treatment protocols for complex scenarios such as poor bone quality or compromised healing conditions. Additionally, considerations such as battery lifespan, structural integrity, and long-term biocompatibility of embedded electronics remain important factors when evaluating their broader clinical adoption.
Would You Put a Battery in Your Mouth?
While the concept of embedding an active electromagnetic system within a healing abutment may appear innovative, it is important to approach it with clinical caution and critical judgment. Introducing a battery-powered electronic component into the oral cavity raises legitimate concerns regarding long-term safety, reliability, and failure risk in a biologically dynamic and mechanically demanding environment. Issues such as battery degradation, potential leakage, sterilization challenges, and the inability to easily service or replace the device once installed should not be overlooked. Moreover, given the current lack of robust long-term clinical evidence demonstrating clear superiority over conventional healing protocols, the risk–benefit ratio remains questionable. From a practical standpoint, clinicians may find it more prudent to rely on well-established, non-invasive adjuncts that offer flexibility, safety, and reversibility, rather than committing to a fixed, embedded system with limited control and uncertain long-term outcomes.
Difference Between Built-in and Available External PEMF Systems
The fundamental distinction between built-in and external PEMF systems lies in precision versus flexibility. Built-in systems deliver electromagnetic stimulation directly at the implant surface, offering unparalleled targeting and continuous exposure without requiring patient intervention. This makes them particularly effective for influencing early osseointegration within a confined biological environment. In contrast, external PEMF devices—commonly adapted from orthopedic or physiotherapy applications—provide broader field distribution and depend on transcutaneous delivery, which inherently reduces precision due to tissue interference.
On the other hand, external systems offer significantly greater control over treatment parameters, including adjustable frequency, intensity, and session duration. They are non-invasive, reusable, and do not require modification of implant components, making them more versatile across different clinical indications. The trade-off is reduced localization and reliance on patient compliance, as repeated sessions are typically necessary. Clinically, built-in systems prioritize convenience and targeted therapy, while external systems emphasize adaptability and operator control.
What If We Made an External PEMF Machine for Improving Oral Surgery Outcomes
Designing an external PEMF system specifically for oral and implant surgery would require a shift from generalized physiotherapy devices toward highly localized, dental-specific engineering. Such a system would need to deliver controlled electromagnetic fields within a narrow anatomical zone—ideally targeting the implant site through the cheek or submandibular region—while maintaining sufficient field strength at the bone level despite soft tissue attenuation. Achieving this would likely involve custom-designed applicators, optimized coil geometry, and possibly higher-frequency ranges than those used in conventional orthopedic PEMF devices.
In addition, a purpose-built dental PEMF unit would need precise control over parameters such as frequency (potentially in the kHz range), intensity in the microtesla-to-millitesla spectrum, and ultra-low duty cycles to mimic experimental conditions shown to influence cellular behavior. Integration with digital workflows—such as guided implant placement or patient-specific treatment protocols—could further enhance outcomes. However, the challenge lies in balancing technical sophistication with clinical practicality, ensuring that such a device remains user-friendly, reproducible, and economically viable for routine dental practice.
PEMF as an Anti-Inflammatory and Pain Reliever for Dentists Suffering from Neck and Back Pain
Beyond its applications in implant dentistry, PEMF therapy has gained attention as a non-pharmacological modality for musculoskeletal pain management, particularly among dental professionals. Dentists are highly prone to chronic neck and back pain due to prolonged static postures, repetitive movements, and ergonomic strain during clinical procedures. PEMF has been shown to modulate inflammatory pathways, reduce cytokine activity, and improve microcirculation, all of which contribute to decreased pain perception and enhanced tissue recovery.
When applied through external devices such as wearable coils or localized pads, PEMF can provide targeted relief to affected muscle groups without systemic side effects. Regular use may help reduce muscle stiffness, improve range of motion, and support long-term spinal health. While not a replacement for ergonomic corrections or physical therapy, PEMF represents a valuable adjunct for managing occupational strain, offering dentists a practical tool to maintain physical well-being and clinical performance over time.
Conclusion
Pulsed Electromagnetic Field therapy represents a scientifically grounded and biologically plausible approach to enhancing implant healing. While early clinical data indicate potential benefits in improving implant stability and modulating inflammation, the current body of evidence remains insufficient for widespread clinical adoption as a standard of care.
Future research should focus on long-term outcomes, standardized treatment protocols, and independent validation to determine whether PEMF can transition from an experimental adjunct to a routine component of implant dentistry.
Frequently Asked Questions (FAQ)
1. What is PEMF therapy in implant dentistry?
PEMF therapy involves the use of pulsed electromagnetic waves to stimulate bone and soft tissue healing around dental implants, to accelerate the osseointegration process.
2. Does PEMF improve implant success rates?
Current evidence suggests improvement in early implant stability, but there is insufficient data to confirm long-term increases in survival rates.
3. Is PEMF safe for all patients?
It is generally safe, but contraindicated in patients with pacemakers or certain electronic medical devices.
4. How long is PEMF therapy applied after implant placement?
Most protocols focus on the first 2–8 weeks, which represent the critical phase of osseointegration.
5. Can PEMF replace conventional implant protocols?
No, it should be considered an adjunctive therapy rather than a replacement for established surgical and prosthetic protocols.
6. Is there strong evidence supporting its routine use?
Not yet. While promising, current evidence is still limited and requires further validation.
7. What is the main clinical benefit of PEMF?
The primary benefit appears to be acceleration of early healing and improvement in initial implant stability.
References:
Recent Articles




































Abstract and Historical Background
Pulsed Electromagnetic Field (PEMF) therapy refers to the application of low-frequency electromagnetic waves delivered in controlled pulses to stimulate biological tissues. Originally developed in the mid-20th century, PEMF gained medical acceptance after its successful use in enhancing bone healing and treating non-union fractures. Regulatory approval in orthopedic medicine, “particularly for delayed fracture healing”, established PEMF as a credible adjunctive therapy grounded in biophysical principles.
The transition of PEMF into dentistry began as clinicians and researchers explored its potential to accelerate osseointegration and improve peri-implant healing. Early experimental studies in the late 1990s and early 2000s demonstrated that electromagnetic stimulation could influence osteoblastic activity and bone remodeling, prompting interest in its application around dental implants. Over time, this evolved into the development of localized delivery systems designed to target peri-implant tissues during the critical healing phase.
Mechanism of Action
The biological effects of PEMF are mediated through complex cellular and molecular pathways. At the cellular level, PEMF influences transmembrane ion exchange, particularly calcium ion channels, which play a crucial role in signal transduction and cellular metabolism.
Key mechanisms include:
- Stimulation of Osteoblast Activity: PEMF enhances proliferation and differentiation of osteoblasts, increasing the production of bone matrix proteins such as collagen type I.
- Upregulation of Growth Factors: Exposure to electromagnetic fields promotes the expression of bone morphogenetic proteins (BMPs), vascular endothelial growth factor (VEGF), and transforming growth factor-beta (TGF-β).
- Enhanced Angiogenesis: Improved microvascular formation supports nutrient delivery and accelerates healing.
- Anti-inflammatory Effects: PEMF has been shown to modulate inflammatory cytokines, reducing levels of TNF-α and IL-1β during early healing.
- Improved Cellular Energy Metabolism: Increased ATP production contributes to faster tissue regeneration.
These mechanisms collectively contribute to enhanced bone formation and remodeling, particularly during the early stages of implant healing.
Effect of PEMF on Peri-Implant Tissues
The peri-implant environment consists of both hard and soft tissues that are critical for long-term implant success. PEMF appears to exert beneficial effects on both components:
1. Bone Tissue (Osseointegration)
Clinical and preclinical studies suggest that PEMF can improve early implant stability, typically measured using resonance frequency analysis (RFA) and implant stability quotient (ISQ) values. Increased bone-to-implant contact (BIC) has also been observed in animal models, indicating enhanced osseointegration.
The primary benefit appears during the early healing phase (first 2–8 weeks), where accelerated bone formation may reduce the risk of early implant failure.
2. Soft Tissue Healing
PEMF may enhance fibroblast proliferation and collagen synthesis, contributing to improved soft tissue sealing around implants. This biological seal is essential in preventing bacterial infiltration and peri-implant inflammation.
3. Inflammatory Modulation
Reduced inflammatory markers in peri-implant crevicular fluid have been reported, suggesting a more controlled healing response. This may be particularly beneficial in patients with compromised healing capacity.
Side Effects and Safety Considerations
PEMF therapy is generally considered safe when used within established parameters. However, several considerations should be acknowledged:
- Minimal Adverse Effects: Most studies report no significant side effects when PEMF is applied at therapeutic levels.
- Contraindications: Patients with pacemakers or other electronic implants may be at risk of electromagnetic interference.
- Thermal Effects: Although rare, improper calibration may lead to mild localized heating.
- Long-Term Data Limitations: There is limited evidence regarding prolonged or repeated exposure in dental applications.
Overall, PEMF demonstrates a favorable safety profile, but cautious patient selection remains essential.
Pros and Cons of Existing Studies in Implant Dentistry
Advantages of Current Evidence
- Presence of Randomized Controlled Trials (RCTs): Some clinical trials provide structured comparisons with control groups.
- Consistent Early-Phase Benefits: Multiple studies report improved implant stability during early healing.
- Biological Plausibility: Strong mechanistic support from in vitro and animal studies.
- Reproducibility in Preclinical Models: Consistent findings across different experimental setups.
Limitations of Current Evidence
- Small Sample Sizes: The only clinical study I found involved limited patient numbers (19 patients), reducing statistical power.
- Short Follow-Up Periods: The study focused on early healing without long-term outcomes.
- Use of Surrogate Endpoints: Reliance on ISQ values rather than implant survival rates.
- Potential Bias: The study is industry-supported, raising concerns about neutrality and conflicts of interest.
- Lack of Standardization: Variability in frequency, intensity, and duration of PEMF application.
These limitations highlight the need for large-scale, independent, multi-center trials to validate current findings.
Is It Wise to Use a Battery Inside an Abutment for PEMF Delivery?
The concept of integrating a power source within a healing abutment introduces both innovation and complexity. From an engineering and clinical perspective, several factors must be considered:
- Advantages:
- Localized delivery directly at the implant site
- Continuous stimulation without patient compliance dependency
- Elimination of external devices
- Concerns:
- Battery reliability and lifespan
- Risk of device failure within the oral environment
- Sterilization and biocompatibility challenges
- Increased cost compared to conventional abutments
- Lack of long-term safety data for embedded electronics
While the concept is technologically appealing, its routine clinical adoption requires further validation, particularly regarding durability and safety.
Properties of the Built-in PEMF
Built-in PEMF systems are engineered as smart healing components that integrate directly with the implant interface, allowing electromagnetic stimulation to be delivered precisely where osseointegration occurs. This localized delivery enables continuous, low-intensity field exposure throughout the critical early healing phase, without relying on patient compliance. The therapeutic concept is based on maintaining a stable electromagnetic microenvironment that supports osteoblastic activity, angiogenesis, and modulation of early inflammatory responses. Because the energy source and coil are embedded within the abutment structure, the system achieves high spatial accuracy—typically within a few millimeters of the peri-implant bone—something external devices struggle to replicate.
However, these systems operate with predefined electromagnetic parameters, meaning clinicians have limited ability to adjust frequency, intensity, or duty cycle based on individual cases. While this standardization ensures consistency, it reduces flexibility in tailoring treatment protocols for complex scenarios such as poor bone quality or compromised healing conditions. Additionally, considerations such as battery lifespan, structural integrity, and long-term biocompatibility of embedded electronics remain important factors when evaluating their broader clinical adoption.
Would You Put a Battery in Your Mouth?
While the concept of embedding an active electromagnetic system within a healing abutment may appear innovative, it is important to approach it with clinical caution and critical judgment. Introducing a battery-powered electronic component into the oral cavity raises legitimate concerns regarding long-term safety, reliability, and failure risk in a biologically dynamic and mechanically demanding environment. Issues such as battery degradation, potential leakage, sterilization challenges, and the inability to easily service or replace the device once installed should not be overlooked. Moreover, given the current lack of robust long-term clinical evidence demonstrating clear superiority over conventional healing protocols, the risk–benefit ratio remains questionable. From a practical standpoint, clinicians may find it more prudent to rely on well-established, non-invasive adjuncts that offer flexibility, safety, and reversibility, rather than committing to a fixed, embedded system with limited control and uncertain long-term outcomes.
Difference Between Built-in and Available External PEMF Systems
The fundamental distinction between built-in and external PEMF systems lies in precision versus flexibility. Built-in systems deliver electromagnetic stimulation directly at the implant surface, offering unparalleled targeting and continuous exposure without requiring patient intervention. This makes them particularly effective for influencing early osseointegration within a confined biological environment. In contrast, external PEMF devices—commonly adapted from orthopedic or physiotherapy applications—provide broader field distribution and depend on transcutaneous delivery, which inherently reduces precision due to tissue interference.
On the other hand, external systems offer significantly greater control over treatment parameters, including adjustable frequency, intensity, and session duration. They are non-invasive, reusable, and do not require modification of implant components, making them more versatile across different clinical indications. The trade-off is reduced localization and reliance on patient compliance, as repeated sessions are typically necessary. Clinically, built-in systems prioritize convenience and targeted therapy, while external systems emphasize adaptability and operator control.
What If We Made an External PEMF Machine for Improving Oral Surgery Outcomes
Designing an external PEMF system specifically for oral and implant surgery would require a shift from generalized physiotherapy devices toward highly localized, dental-specific engineering. Such a system would need to deliver controlled electromagnetic fields within a narrow anatomical zone—ideally targeting the implant site through the cheek or submandibular region—while maintaining sufficient field strength at the bone level despite soft tissue attenuation. Achieving this would likely involve custom-designed applicators, optimized coil geometry, and possibly higher-frequency ranges than those used in conventional orthopedic PEMF devices.
In addition, a purpose-built dental PEMF unit would need precise control over parameters such as frequency (potentially in the kHz range), intensity in the microtesla-to-millitesla spectrum, and ultra-low duty cycles to mimic experimental conditions shown to influence cellular behavior. Integration with digital workflows—such as guided implant placement or patient-specific treatment protocols—could further enhance outcomes. However, the challenge lies in balancing technical sophistication with clinical practicality, ensuring that such a device remains user-friendly, reproducible, and economically viable for routine dental practice.
PEMF as an Anti-Inflammatory and Pain Reliever for Dentists Suffering from Neck and Back Pain
Beyond its applications in implant dentistry, PEMF therapy has gained attention as a non-pharmacological modality for musculoskeletal pain management, particularly among dental professionals. Dentists are highly prone to chronic neck and back pain due to prolonged static postures, repetitive movements, and ergonomic strain during clinical procedures. PEMF has been shown to modulate inflammatory pathways, reduce cytokine activity, and improve microcirculation, all of which contribute to decreased pain perception and enhanced tissue recovery.
When applied through external devices such as wearable coils or localized pads, PEMF can provide targeted relief to affected muscle groups without systemic side effects. Regular use may help reduce muscle stiffness, improve range of motion, and support long-term spinal health. While not a replacement for ergonomic corrections or physical therapy, PEMF represents a valuable adjunct for managing occupational strain, offering dentists a practical tool to maintain physical well-being and clinical performance over time.
Conclusion
Pulsed Electromagnetic Field therapy represents a scientifically grounded and biologically plausible approach to enhancing implant healing. While early clinical data indicate potential benefits in improving implant stability and modulating inflammation, the current body of evidence remains insufficient for widespread clinical adoption as a standard of care.
Future research should focus on long-term outcomes, standardized treatment protocols, and independent validation to determine whether PEMF can transition from an experimental adjunct to a routine component of implant dentistry.
Frequently Asked Questions (FAQ)
1. What is PEMF therapy in implant dentistry?
PEMF therapy involves the use of pulsed electromagnetic waves to stimulate bone and soft tissue healing around dental implants, to accelerate the osseointegration process.
2. Does PEMF improve implant success rates?
Current evidence suggests improvement in early implant stability, but there is insufficient data to confirm long-term increases in survival rates.
3. Is PEMF safe for all patients?
It is generally safe, but contraindicated in patients with pacemakers or certain electronic medical devices.
4. How long is PEMF therapy applied after implant placement?
Most protocols focus on the first 2–8 weeks, which represent the critical phase of osseointegration.
5. Can PEMF replace conventional implant protocols?
No, it should be considered an adjunctive therapy rather than a replacement for established surgical and prosthetic protocols.
6. Is there strong evidence supporting its routine use?
Not yet. While promising, current evidence is still limited and requires further validation.
7. What is the main clinical benefit of PEMF?
The primary benefit appears to be acceleration of early healing and improvement in initial implant stability.
References:
Recent Articles
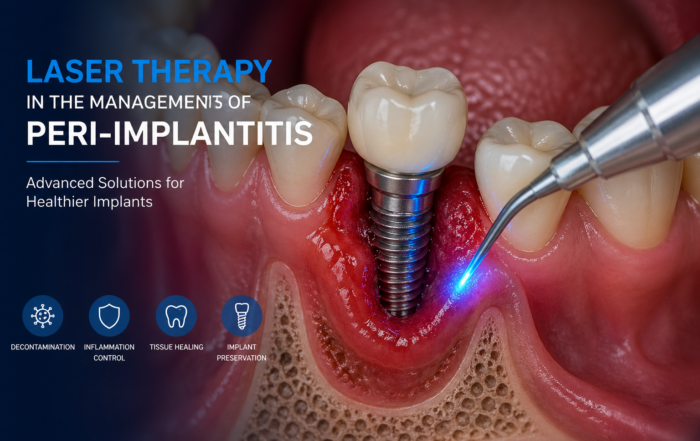
Laser Therapy in the Management of Peri-Implantitis
Laser Therapy in the Management of Peri-Implantitis Laser technology has become an increasingly valuable adjunct in the treatment of peri-implant diseases, particularly peri-implantitis. Its [...]
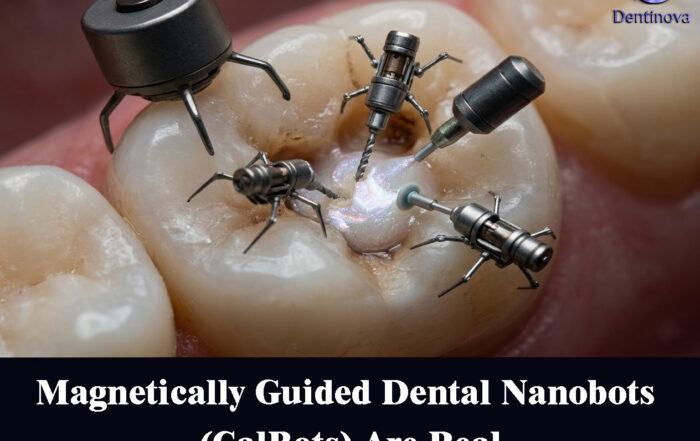
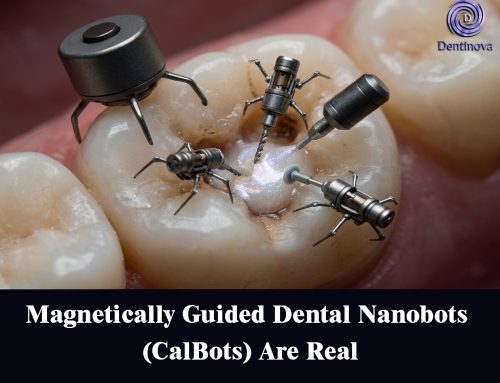
Magnetically Guided Dental Nanobots (CalBots) Are Real
Magnetically Guided Dental Nanobots (CalBots) Are Real The concept of nanobots in dentistry has long been associated with futuristic speculation. However, recent peer-reviewed research [...]

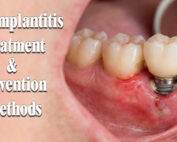
Peri-Implantitis Treatment & Prevention Methods
Peri-Implantitis Treatment & Prevention Methods Peri-implantitis remains one of the most significant biological complications affecting dental implants, posing a serious threat to long-term implant [...]
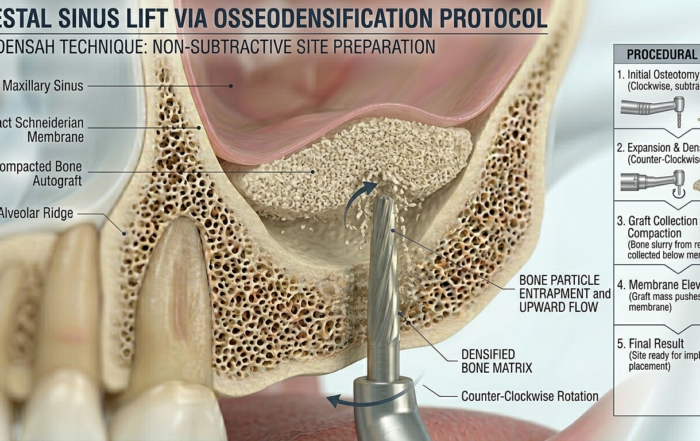
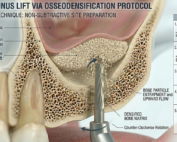
Latest Sinus Lifting Techniques in Modern Implant Dentistry
Latest Sinus Lifting Techniques in Modern Implant Dentistry A Comprehensive Clinical Review Introduction to Sinus Lifting in Implantology Sinus lifting, or maxillary sinus floor [...]

Biomechanics of the Triple Abutment & BOPiT Concept
Dental Biomechanics · Implant Science · Clinical Evidence Biomechanics of the Triple Abutment & BOPiT Concept How a saddle-shaped mathematical surface is rewriting the rules of load distribution [...]

The Woman Who Proved One Implant Could Hold Three Crowns
The Woman Who Proved One Implant Could Hold Three Crowns While the dental establishment looked away, Dr. Luciana Colepícolo spent 12 years building the [...]

{kind=link}
{kind=link}
{kind=link}