

Snoring and Obstructive Sleep Apnea: Symptoms & Treatment
The Expanding Role of Dentists in Early Detection
Introduction
Snoring is a respiratory sound produced during sleep due to vibration of the oropharyngeal soft tissues when airflow becomes partially obstructed. While often dismissed as harmless, chronic snoring is one of the most common early warning signs of obstructive sleep apnea (OSA) — a serious sleep-related breathing disorder with systemic health consequences.
Obstructive sleep apnea affects millions of adults worldwide and is characterized by repeated episodes of partial or complete upper airway collapse during sleep. These events result in intermittent hypoxia, sleep fragmentation, and long-term cardiovascular and metabolic risks. Despite its prevalence, OSA remains significantly underdiagnosed.
Understanding the relationship between snoring and obstructive sleep apnea is critical for early detection, appropriate referral, and effective treatment.
What Is Obstructive Sleep Apnea (OSA)?
Obstructive sleep apnea (OSA) is a chronic sleep disorder defined by recurrent airway obstruction during sleep, leading to reduced or completely blocked airflow.
Severity is measured using the Apnea–Hypopnea Index (AHI) — the average number of apnea and hypopnea events per hour of sleep.
Major Risk Factors for OSA:
Obesity (BMI > 30 kg/m²)
Large neck circumference (> 41 cm)
Increased waist circumference
Advancing age
Craniofacial airway narrowing
Smoking
Postmenopausal status
Genetic predisposition
OSA is associated with cardiovascular disease, hypertension, daytime sleepiness, cognitive impairment, and reduced quality of life.
Snoring: What Causes It and Why It Matters
Snoring occurs when relaxed soft tissues — including the tongue and soft palate — vibrate as air passes through a narrowed airway during sleep.
It is more likely to occur when:
Muscle tone decreases in deeper sleep stages
The tongue falls posteriorly
Airway anatomy is constricted
Excess adipose tissue narrows the pharyngeal space
While occasional snoring may be benign, persistent or loud snoring is strongly correlated with obstructive sleep apnea severity.
Clinical Findings in Individuals Who Snore:
Higher body mass index (BMI)
Larger neck circumference
Greater waist and hip circumference
Higher AHI scores
Increased hypopneas and apneas
Lower minimum oxygen saturation
Reduced deep sleep (N3 stage)
Greater daytime sleepiness (higher ESS scores)
Snoring should therefore be considered a clinical risk marker for sleep-disordered breathing.
Is Snoring a Disease?
Snoring itself is not classified as a disease. However, it is a primary symptom of obstructive sleep apnea and may indicate underlying airway instability.
Research demonstrates that individuals who report habitual snoring are significantly more likely to exhibit objective polysomnographic evidence of OSA, including elevated AHI values and oxygen desaturation.
Ignoring chronic snoring may delay diagnosis of moderate to severe obstructive sleep apnea.
Evidence from Clinical Study
A retrospective cross-sectional study evaluated 795 adults (aged 18–75 years) who underwent overnight polysomnography.
Key Findings:
73% reported subjective snoring
Snorers had significantly higher BMI and body circumferences
Snorers were older on average
Higher AHI values were observed in both REM and non-REM sleep
Increased obstructive, central, and mixed apneas
Lower minimum oxygen saturation
Greater daytime sleepiness
Independent Predictors of Snoring:
Multivariate logistic regression identified:
Body Mass Index (BMI)
Apnea–Hypopnea Index (AHI)
Age
Sex was not an independent predictor.
These findings confirm a strong association between snoring and obstructive sleep apnea severity.
Management of Snoring and Obstructive Sleep Apnea
Treatment depends on severity and patient-specific risk factors.
1. Lifestyle Modification
Weight reduction
Smoking cessation
Alcohol reduction
Positional therapy
Weight loss alone can significantly reduce snoring intensity and OSA severity.
2. CPAP Therapy
Continuous Positive Airway Pressure (CPAP) remains the gold standard for moderate to severe OSA. It prevents airway collapse by delivering pressurized airflow during sleep.
However, intolerance and compliance issues are common.
3. Oral Appliance Therapy (Dental Sleep Medicine)
For primary snoring and mild to moderate obstructive sleep apnea, oral appliances provide an effective non-surgical alternative.
Mandibular advancement devices (MADs) and tongue-retaining devices (TRDs):
Advance the lower jaw forward
Increase airway patency
Reduce upper airway collapse
Improve oxygen saturation
Decrease snoring intensity
Oral appliances are particularly valuable for patients intolerant to CPAP therapy.
Meet the Silencer: Modern Oral Appliance Solutions
Advanced custom-fabricated mandibular advancement systems — often referred to as “silent” sleep appliances — are designed to stabilize the airway comfortably.
These intraoral devices:
Are worn during sleep
Gently reposition the mandible
Reduce airway obstruction
Minimize vibration of soft tissues
Significantly decrease snoring
For appropriately selected patients, oral appliance therapy can substantially improve sleep quality and reduce OSA symptoms.

Illustration of the use of an oral appliance that keeps the airway open
Illustration of the use of an oral appliance that keeps the airway open
 Fabrication For Sleep Apnea")
Snore Guard ( Silencer ) Fabrication For Sleep Apnea
Illustration of the use of an oral appliance that keeps the airway open
Oral Health Implications of Untreated OSA
Obstructive sleep apnea has important dental and oral health consequences:
Mouth breathing
Xerostomia
Altered salivary composition
Increased inflammatory burden
Gingivitis and periodontitis
Enamel erosion
Increased caries risk
Tooth wear and bruxism
Effective management of OSA may improve salivary flow and reduce xerostomia-related complications.
The Role of Dentists in Snoring and OSA Screening
Dental professionals are uniquely positioned to identify patients at risk for obstructive sleep apnea.
During routine examinations, dentists can assess:
BMI and neck circumference
Craniofacial airway anatomy
Bruxism and tooth wear
Xerostomia
Periodontal inflammation
Validated screening tools such as:
STOP questionnaire
Epworth Sleepiness Scale (ESS)
can be incorporated into dental practice to identify high-risk individuals and facilitate referral for polysomnography (PSG), the diagnostic gold standard.
Early detection improves systemic health outcomes and expands the role of dental sleep medicine.
Strengths and Limitations of the Study
Strengths:
Large sample size (795 participants)
Objective polysomnography-based diagnosis
Validated screening tools
Multivariate statistical analysis
Limitations:
Self-reported snoring
Single-center design
Cross-sectional structure (no causal inference)
Conclusion
Snoring is not merely a social inconvenience — it is strongly associated with obstructive sleep apnea severity.
Higher BMI, elevated AHI values, and increasing age are the strongest predictors of snoring and OSA risk.
Given their routine access to airway-related anatomy, dentists play a critical role in early identification and management of sleep-disordered breathing. Integrating structured screening protocols into dental practice may significantly improve detection rates and patient outcomes.
Frequently Asked Questions (FAQ)
1. Is snoring always a sign of obstructive sleep apnea?
No, but persistent snoring is strongly associated with elevated AHI values, oxygen desaturation, and increased apnea events, making it an important clinical warning sign.
2. What are the strongest predictors of OSA?
Body mass index (BMI), apnea–hypopnea index (AHI), and age are the strongest independent predictors.
3. How does obesity increase OSA risk?
Excess adipose tissue around the upper airway increases collapsibility during sleep, leading to airflow obstruction and intermittent hypoxia.
4. What sleep study findings are common in snorers?
Higher AHI, increased obstructive and mixed apneas, reduced deep sleep, lower oxygen saturation, and higher daytime sleepiness scores.
5. Can oral appliances replace CPAP?
For mild to moderate OSA and primary snoring, mandibular advancement devices can be an effective alternative, particularly for CPAP-intolerant patients.
6. How can dentists help detect OSA?
By evaluating airway anatomy, BMI, oral manifestations, and using validated screening tools such as STOP and ESS questionnaires.
Recent Articles




































Introduction
Snoring is a respiratory sound produced during sleep due to vibration of the oropharyngeal soft tissues when airflow becomes partially obstructed. While often dismissed as harmless, chronic snoring is one of the most common early warning signs of obstructive sleep apnea (OSA) — a serious sleep-related breathing disorder with systemic health consequences.
Obstructive sleep apnea affects millions of adults worldwide and is characterized by repeated episodes of partial or complete upper airway collapse during sleep. These events result in intermittent hypoxia, sleep fragmentation, and long-term cardiovascular and metabolic risks. Despite its prevalence, OSA remains significantly underdiagnosed.
Understanding the relationship between snoring and obstructive sleep apnea is critical for early detection, appropriate referral, and effective treatment.
What Is Obstructive Sleep Apnea (OSA)?
Obstructive sleep apnea (OSA) is a chronic sleep disorder defined by recurrent airway obstruction during sleep, leading to reduced or completely blocked airflow.
Severity is measured using the Apnea–Hypopnea Index (AHI) — the average number of apnea and hypopnea events per hour of sleep.
Major Risk Factors for OSA:
Obesity (BMI > 30 kg/m²)
Large neck circumference (> 41 cm)
Increased waist circumference
Advancing age
Craniofacial airway narrowing
Smoking
Postmenopausal status
Genetic predisposition
OSA is associated with cardiovascular disease, hypertension, daytime sleepiness, cognitive impairment, and reduced quality of life.
Snoring: What Causes It and Why It Matters
Snoring occurs when relaxed soft tissues — including the tongue and soft palate — vibrate as air passes through a narrowed airway during sleep.
It is more likely to occur when:
Muscle tone decreases in deeper sleep stages
The tongue falls posteriorly
Airway anatomy is constricted
Excess adipose tissue narrows the pharyngeal space
While occasional snoring may be benign, persistent or loud snoring is strongly correlated with obstructive sleep apnea severity.
Clinical Findings in Individuals Who Snore:
Higher body mass index (BMI)
Larger neck circumference
Greater waist and hip circumference
Higher AHI scores
Increased hypopneas and apneas
Lower minimum oxygen saturation
Reduced deep sleep (N3 stage)
Greater daytime sleepiness (higher ESS scores)
Snoring should therefore be considered a clinical risk marker for sleep-disordered breathing.
Is Snoring a Disease?
Snoring itself is not classified as a disease. However, it is a primary symptom of obstructive sleep apnea and may indicate underlying airway instability.
Research demonstrates that individuals who report habitual snoring are significantly more likely to exhibit objective polysomnographic evidence of OSA, including elevated AHI values and oxygen desaturation.
Ignoring chronic snoring may delay diagnosis of moderate to severe obstructive sleep apnea.
Evidence from Clinical Study
A retrospective cross-sectional study evaluated 795 adults (aged 18–75 years) who underwent overnight polysomnography.
Key Findings:
73% reported subjective snoring
Snorers had significantly higher BMI and body circumferences
Snorers were older on average
Higher AHI values were observed in both REM and non-REM sleep
Increased obstructive, central, and mixed apneas
Lower minimum oxygen saturation
Greater daytime sleepiness
Independent Predictors of Snoring:
Multivariate logistic regression identified:
Body Mass Index (BMI)
Apnea–Hypopnea Index (AHI)
Age
Sex was not an independent predictor.
These findings confirm a strong association between snoring and obstructive sleep apnea severity.
Management of Snoring and Obstructive Sleep Apnea
Treatment depends on severity and patient-specific risk factors.
1. Lifestyle Modification
Weight reduction
Smoking cessation
Alcohol reduction
Positional therapy
Weight loss alone can significantly reduce snoring intensity and OSA severity.
2. CPAP Therapy
Continuous Positive Airway Pressure (CPAP) remains the gold standard for moderate to severe OSA. It prevents airway collapse by delivering pressurized airflow during sleep.
However, intolerance and compliance issues are common.
3. Oral Appliance Therapy (Dental Sleep Medicine)
For primary snoring and mild to moderate obstructive sleep apnea, oral appliances provide an effective non-surgical alternative.
Mandibular advancement devices (MADs) and tongue-retaining devices (TRDs):
Advance the lower jaw forward
Increase airway patency
Reduce upper airway collapse
Improve oxygen saturation
Decrease snoring intensity
Oral appliances are particularly valuable for patients intolerant to CPAP therapy.
Meet the Silencer: Modern Oral Appliance Solutions
Advanced custom-fabricated mandibular advancement systems — often referred to as “silent” sleep appliances — are designed to stabilize the airway comfortably.
These intraoral devices:
Are worn during sleep
Gently reposition the mandible
Reduce airway obstruction
Minimize vibration of soft tissues
Significantly decrease snoring
For appropriately selected patients, oral appliance therapy can substantially improve sleep quality and reduce OSA symptoms.
Illustration of the use of an oral appliance that keeps the airway open
Illustration of the use of an oral appliance that keeps the airway open
Snore Guard ( Silencer ) Fabrication For Sleep Apnea
Illustration of the use of an oral appliance that keeps the airway open
Oral Health Implications of Untreated OSA
Obstructive sleep apnea has important dental and oral health consequences:
Mouth breathing
Xerostomia
Altered salivary composition
Increased inflammatory burden
Gingivitis and periodontitis
Enamel erosion
Increased caries risk
Tooth wear and bruxism
Effective management of OSA may improve salivary flow and reduce xerostomia-related complications.
The Role of Dentists in Snoring and OSA Screening
Dental professionals are uniquely positioned to identify patients at risk for obstructive sleep apnea.
During routine examinations, dentists can assess:
BMI and neck circumference
Craniofacial airway anatomy
Bruxism and tooth wear
Xerostomia
Periodontal inflammation
Validated screening tools such as:
STOP questionnaire
Epworth Sleepiness Scale (ESS)
can be incorporated into dental practice to identify high-risk individuals and facilitate referral for polysomnography (PSG), the diagnostic gold standard.
Early detection improves systemic health outcomes and expands the role of dental sleep medicine.
Strengths and Limitations of the Study
Strengths:
Large sample size (795 participants)
Objective polysomnography-based diagnosis
Validated screening tools
Multivariate statistical analysis
Limitations:
Self-reported snoring
Single-center design
Cross-sectional structure (no causal inference)
Conclusion
Snoring is not merely a social inconvenience — it is strongly associated with obstructive sleep apnea severity.
Higher BMI, elevated AHI values, and increasing age are the strongest predictors of snoring and OSA risk.
Given their routine access to airway-related anatomy, dentists play a critical role in early identification and management of sleep-disordered breathing. Integrating structured screening protocols into dental practice may significantly improve detection rates and patient outcomes.
Frequently Asked Questions (FAQ)
1. Is snoring always a sign of obstructive sleep apnea?
No, but persistent snoring is strongly associated with elevated AHI values, oxygen desaturation, and increased apnea events, making it an important clinical warning sign.
2. What are the strongest predictors of OSA?
Body mass index (BMI), apnea–hypopnea index (AHI), and age are the strongest independent predictors.
3. How does obesity increase OSA risk?
Excess adipose tissue around the upper airway increases collapsibility during sleep, leading to airflow obstruction and intermittent hypoxia.
4. What sleep study findings are common in snorers?
Higher AHI, increased obstructive and mixed apneas, reduced deep sleep, lower oxygen saturation, and higher daytime sleepiness scores.
5. Can oral appliances replace CPAP?
For mild to moderate OSA and primary snoring, mandibular advancement devices can be an effective alternative, particularly for CPAP-intolerant patients.
6. How can dentists help detect OSA?
By evaluating airway anatomy, BMI, oral manifestations, and using validated screening tools such as STOP and ESS questionnaires.
Recent Articles
Magnetically Guided Dental Nanobots (CalBots) Are Real
Magnetically Guided Dental Nanobots (CalBots) Are Real The concept of nanobots in dentistry has long been associated with futuristic speculation. However, recent peer-reviewed research [...]

Peri-Implantitis Treatment & Prevention Methods
Peri-Implantitis Treatment & Prevention Methods Peri-implantitis remains one of the most significant biological complications affecting dental implants, posing a serious threat to long-term implant [...]
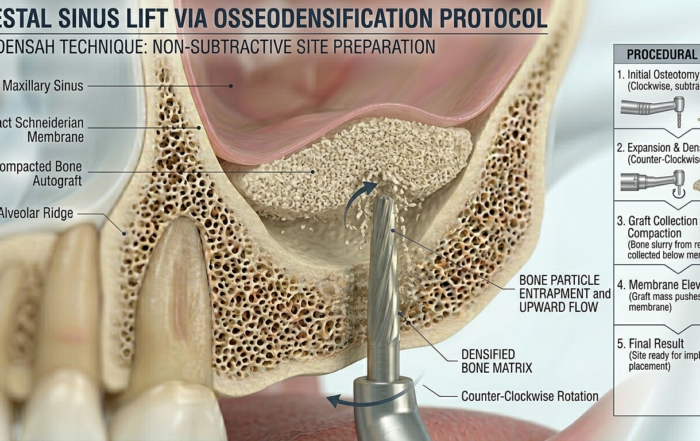
Latest Sinus Lifting Techniques in Modern Implant Dentistry
Latest Sinus Lifting Techniques in Modern Implant Dentistry A Comprehensive Clinical Review Introduction to Sinus Lifting in Implantology Sinus lifting, or maxillary sinus floor [...]

Biomechanics of the Triple Abutment & BOPiT Concept
Dental Biomechanics · Implant Science · Clinical Evidence Biomechanics of the Triple Abutment & BOPiT Concept How a saddle-shaped mathematical surface is rewriting the rules of load distribution [...]

The Woman Who Proved One Implant Could Hold Three Crowns
The Woman Who Proved One Implant Could Hold Three Crowns While the dental establishment looked away, Dr. Luciana Colepícolo spent 12 years building the [...]
ENPP1, The Molecular Brake That Limits Tissue Healing
ENPP1, The Molecular Brake That Limits Tissue Healing Introduction: A New Biological Barrier to Dental Regeneration Meet ENPP1—a protein most dentists have never heard [...]