

Cracked Tooth Diagnosis in 2025: From Clinical Tests to CBCT
Introduction: Why Early Cracked Tooth Diagnosis Matters
Diagnosing a cracked tooth is a challenge in everyday practice. The clinical presentation is highly variable, ranging from vague biting discomfort to acute pain on release, or even completely asymptomatic in early stages. If left undiagnosed, cracks can propagate, leading to pulpal inflammation, vertical root fractures, and eventual tooth loss. Accurate and timely diagnosis directly impacts prognosis, treatment planning, and patient quality of life.
Despite advances in technology, clinicians still grapple with differentiating cracked teeth from other common dental pain sources like pulpal pathosis or periodontal disease. The complexities of crack morphology, orientation, and depth require a thoughtful, evidence-based diagnostic approach that includes both traditional clinical tests and advanced imaging. SpringerLink
Traditional Clinical Tests
1. Bite and Occlusal Tests
A bite test — using a tooth sleuth or similar device — can be revealing. Pain upon biting, particularly on release, often signifies a crack that flexes the crown segments. However, these tests are subjective and vary with patient cooperation and interpretation.
2. Transillumination and Visual Inspection
Transillumination assists in highlighting surface cracks by revealing discontinuities in light transmission through enamel. Among standard visual tests, transillumination showed the highest diagnostic accuracy (65.3%) and sensitivity (68.8%) compared to other visual aids like macrophotography or microscopes when validated against micro-CT standards in vitro. PubMed
Even so, visual methods alone cannot definitively diagnose cracked teeth in all cases and may miss subsurface or very fine cracks. Clinical experience appears to correlate with better diagnostic accuracy, but no single visual test is sufficient in isolation. PubMed
3. Periodontal Probing
A localized deep periodontal pocket adjacent to a suspected crack suggests significant extension of the crack below the gingival margin — a critical finding that may distinguish between a simple crack and a split tooth. Careful probing is essential, but must be executed gently to avoid propagating an existing crack. PubMed Central
4. Vitality and Sensibility Tests
Cold or electric pulp testing may help determine pulpal involvement, although these tests are not specific for cracks and should be interpreted in the context of all clinical findings.
5. Dye Tests and Staining
Dye application (e.g., methylene blue or gentian violet) can sometimes highlight fracture lines. However, this method requires time for stain uptake and impacts restorative planning if provisional restorations are placed. PubMed Central
Imaging: From Bitewings & Periapicals to 3D Volumes
Limitations of Conventional 2D Imaging
Periapical and bitewing radiographs are often the first imaging modality used in diagnosis. While effective for caries and alveolar bone pathology, they are limited in detecting narrow crack lines, especially those oriented mesiodistally, and they may provide a false sense of security when the fracture plane is parallel to the X-ray beam. PubMed Central
CBCT: Advantages and Real-World Accuracy
Cone-beam computed tomography (CBCT) offers three-dimensional visualization of dental structures and can reveal subtle changes in internal anatomy, root fractures, and associated periodontal defects. Recent clinical retrospective studies have shown that CBCT outperforms periapical radiographs in detecting longitudinal fractures and evaluating patterns of bone loss linked to cracked teeth. PubMed
However, the diagnostic role of standard CBCT for early crack detection remains debated. In traditional use, wide cracks may be visualized, but very narrow or superficial cracks often fall below the spatial resolution threshold of many CBCT units. PubMed Central
New Techniques: Contrast-Enhanced CBCT
What Is It?
Contrast-enhanced CBCT refers to the introduction of radiopaque agents into crack lines before scanning to improve visualization. This technique is not yet standard clinical practice but is undergoing active research with promising results.
Evidence from Recent Studies
A 2025 systematic review and meta-analysis found that CBCT with contrast agents significantly improves diagnostic sensitivity and specificity for detecting tooth cracks and fractures. Sensitivity and specificity frequently exceeded 80%, and accuracy improvements — compared with non-enhanced CBCT — ranged as high as 4.4% to more than 70%. Importantly, systemic differences in imaging protocols and contrast media formulations (e.g., sodium iodide combined with dimethyl sulfoxide) influenced performance. PubMed+1
In vitro comparisons of CBCT with and without contrast media showed that cracks largely invisible on routine scans became detectable once contrast was applied. One study reported that CBCT with sodium iodide and dimethyl sulfoxide identified significantly more crack lines than standard CBCT and approached the detection numbers seen with micro-CT — a gold standard in laboratory settings. PubMed+1
Another research line explored combinations of contrast agents (e.g., sodium iodide, ethyl alcohol, ethyl acetate) and discovered that certain mixtures enhanced crack visualization and depth measurements more effectively than others. PubMed
Pros and Cons
Pros:
Enhanced detection of subsurface cracks that are otherwise invisible. PubMed
Potentially improved assessment of crack depth and morphology. PubMed
Can reduce artifacts and improve diagnostic confidence.
Cons:
Many studies remain in vitro, with limited clinical application guidelines. PubMed
Contrast materials may require controlled delivery and vacuum conditions, making in-office translation challenging. PubMed
There are no standardized clinical protocols or widely available contrast products approved for this use as of 2025.
Putting It All Together: A Practical Diagnostic Workflow
A practical, evidence-based approach to diagnosing cracked teeth in 2025 might include:
Clinical History & Symptom Review
Pain and sensitivity to biting and thermal changes.
Rule out temporomandibular, periodontal, or pulpal pathosis.
Initial Clinical Tests
Bite test and occlusal analysis.
Transillumination and visual inspection.
Periodontal probing for isolated deep pockets.
Vitality testing as supportive information.
Conventional Imaging
Periapical and bitewing radiographs to assess bone and root patterns.
Look for subtle periodontal defects or radiolucent lines suggestive of a crack.
3D Imaging
Standard CBCT is used when 2D imaging is inconclusive, but clinical suspicion remains high.
Consider machine settings that optimize spatial resolution.
Review images for subtle hypodense lines, changes in enamel/dentin continuity, and associated bone changes.
Advanced Techniques (Research/Referral)
Contrast-enhanced CBCT can be considered in complex or ambiguous cases, ideally in referral or research settings where protocols exist.
Combine CBCT findings with magnification, staining, and intraoral diagnostic aids.
Integration and Follow-Up
Correlate clinical findings with all imaging modalities.
When in doubt, monitor the patient with close recall intervals or refer to a specialist (endodontist) who can use additional diagnostic tools like operative microscopes and dyes.
Decision Tree (Simplified)
Conclusion
In 2025, diagnosing cracked teeth still requires a multimodal approach. While traditional clinical tests (bite testing, transillumination, probing) remain foundational, 3D imaging with CBCT has become an invaluable adjunct — particularly for complex or unclear cases. Recent research on contrast-enhanced CBCT suggests a significant leap forward in detection accuracy, though clinical implementation awaits standardized protocols and broader validation. PubMed+1
Dentists should combine clinical acumen with an evidence-based imaging strategy to ensure early, accurate detection and improved outcomes for patients with cracked teeth.
Recent Articles





































Introduction: Why Early Cracked Tooth Diagnosis Matters
Diagnosing a cracked tooth is a challenge in everyday practice. The clinical presentation is highly variable, ranging from vague biting discomfort to acute pain on release, or even completely asymptomatic in early stages. If left undiagnosed, cracks can propagate, leading to pulpal inflammation, vertical root fractures, and eventual tooth loss. Accurate and timely diagnosis directly impacts prognosis, treatment planning, and patient quality of life.
Despite advances in technology, clinicians still grapple with differentiating cracked teeth from other common dental pain sources like pulpal pathosis or periodontal disease. The complexities of crack morphology, orientation, and depth require a thoughtful, evidence-based diagnostic approach that includes both traditional clinical tests and advanced imaging. SpringerLink
Traditional Clinical Tests
1. Bite and Occlusal Tests
A bite test — using a tooth sleuth or similar device — can be revealing. Pain upon biting, particularly on release, often signifies a crack that flexes the crown segments. However, these tests are subjective and vary with patient cooperation and interpretation.
2. Transillumination and Visual Inspection
Transillumination assists in highlighting surface cracks by revealing discontinuities in light transmission through enamel. Among standard visual tests, transillumination showed the highest diagnostic accuracy (65.3%) and sensitivity (68.8%) compared to other visual aids like macrophotography or microscopes when validated against micro-CT standards in vitro. PubMed
Even so, visual methods alone cannot definitively diagnose cracked teeth in all cases and may miss subsurface or very fine cracks. Clinical experience appears to correlate with better diagnostic accuracy, but no single visual test is sufficient in isolation. PubMed
3. Periodontal Probing
A localized deep periodontal pocket adjacent to a suspected crack suggests significant extension of the crack below the gingival margin — a critical finding that may distinguish between a simple crack and a split tooth. Careful probing is essential, but must be executed gently to avoid propagating an existing crack. PubMed Central
4. Vitality and Sensibility Tests
Cold or electric pulp testing may help determine pulpal involvement, although these tests are not specific for cracks and should be interpreted in the context of all clinical findings.
5. Dye Tests and Staining
Dye application (e.g., methylene blue or gentian violet) can sometimes highlight fracture lines. However, this method requires time for stain uptake and impacts restorative planning if provisional restorations are placed. PubMed Central
Imaging: From Bitewings & Periapicals to 3D Volumes
Limitations of Conventional 2D Imaging
Periapical and bitewing radiographs are often the first imaging modality used in diagnosis. While effective for caries and alveolar bone pathology, they are limited in detecting narrow crack lines, especially those oriented mesiodistally, and they may provide a false sense of security when the fracture plane is parallel to the X-ray beam. PubMed Central
CBCT: Advantages and Real-World Accuracy
Cone-beam computed tomography (CBCT) offers three-dimensional visualization of dental structures and can reveal subtle changes in internal anatomy, root fractures, and associated periodontal defects. Recent clinical retrospective studies have shown that CBCT outperforms periapical radiographs in detecting longitudinal fractures and evaluating patterns of bone loss linked to cracked teeth. PubMed
However, the diagnostic role of standard CBCT for early crack detection remains debated. In traditional use, wide cracks may be visualized, but very narrow or superficial cracks often fall below the spatial resolution threshold of many CBCT units. PubMed Central
New Techniques: Contrast-Enhanced CBCT
What Is It?
Contrast-enhanced CBCT refers to the introduction of radiopaque agents into crack lines before scanning to improve visualization. This technique is not yet standard clinical practice but is undergoing active research with promising results.
Evidence from Recent Studies
A 2025 systematic review and meta-analysis found that CBCT with contrast agents significantly improves diagnostic sensitivity and specificity for detecting tooth cracks and fractures. Sensitivity and specificity frequently exceeded 80%, and accuracy improvements — compared with non-enhanced CBCT — ranged as high as 4.4% to more than 70%. Importantly, systemic differences in imaging protocols and contrast media formulations (e.g., sodium iodide combined with dimethyl sulfoxide) influenced performance. PubMed+1
In vitro comparisons of CBCT with and without contrast media showed that cracks largely invisible on routine scans became detectable once contrast was applied. One study reported that CBCT with sodium iodide and dimethyl sulfoxide identified significantly more crack lines than standard CBCT and approached the detection numbers seen with micro-CT — a gold standard in laboratory settings. PubMed+1
Another research line explored combinations of contrast agents (e.g., sodium iodide, ethyl alcohol, ethyl acetate) and discovered that certain mixtures enhanced crack visualization and depth measurements more effectively than others. PubMed
Pros and Cons
Pros:
Enhanced detection of subsurface cracks that are otherwise invisible. PubMed
Potentially improved assessment of crack depth and morphology. PubMed
Can reduce artifacts and improve diagnostic confidence.
Cons:
Many studies remain in vitro, with limited clinical application guidelines. PubMed
Contrast materials may require controlled delivery and vacuum conditions, making in-office translation challenging. PubMed
There are no standardized clinical protocols or widely available contrast products approved for this use as of 2025.
Putting It All Together: A Practical Diagnostic Workflow
A practical, evidence-based approach to diagnosing cracked teeth in 2025 might include:
Clinical History & Symptom Review
Pain and sensitivity to biting and thermal changes.
Rule out temporomandibular, periodontal, or pulpal pathosis.
Initial Clinical Tests
Bite test and occlusal analysis.
Transillumination and visual inspection.
Periodontal probing for isolated deep pockets.
Vitality testing as supportive information.
Conventional Imaging
Periapical and bitewing radiographs to assess bone and root patterns.
Look for subtle periodontal defects or radiolucent lines suggestive of a crack.
3D Imaging
Standard CBCT is used when 2D imaging is inconclusive, but clinical suspicion remains high.
Consider machine settings that optimize spatial resolution.
Review images for subtle hypodense lines, changes in enamel/dentin continuity, and associated bone changes.
Advanced Techniques (Research/Referral)
Contrast-enhanced CBCT can be considered in complex or ambiguous cases, ideally in referral or research settings where protocols exist.
Combine CBCT findings with magnification, staining, and intraoral diagnostic aids.
Integration and Follow-Up
Correlate clinical findings with all imaging modalities.
When in doubt, monitor the patient with close recall intervals or refer to a specialist (endodontist) who can use additional diagnostic tools like operative microscopes and dyes.
Decision Tree (Simplified)
Conclusion
In 2025, diagnosing cracked teeth still requires a multimodal approach. While traditional clinical tests (bite testing, transillumination, probing) remain foundational, 3D imaging with CBCT has become an invaluable adjunct — particularly for complex or unclear cases. Recent research on contrast-enhanced CBCT suggests a significant leap forward in detection accuracy, though clinical implementation awaits standardized protocols and broader validation. PubMed+1
Dentists should combine clinical acumen with an evidence-based imaging strategy to ensure early, accurate detection and improved outcomes for patients with cracked teeth.
Recent Articles
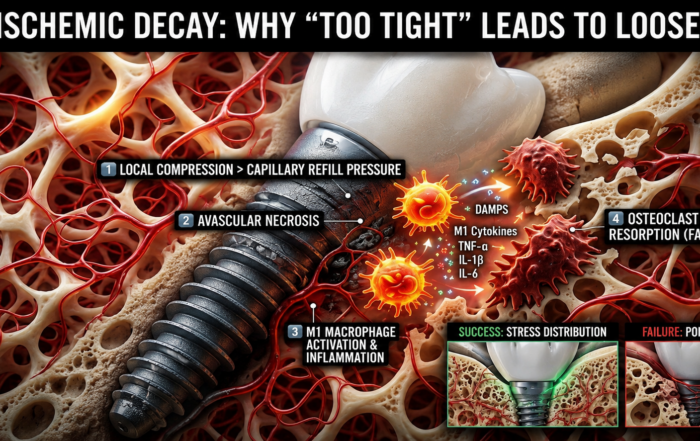
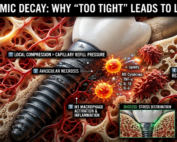
When “Perfectly Tight” Dental Implants Fail
When “Perfectly Tight” Dental Implants Fail The Hidden Role of Ischemic Bone Resorption and Osteoimmune Dysfunction In modern dental implantology, achieving high primary [...]

The Bicuspidization Protocol: Engineering Meets Survival
The Bicuspidization Protocol: Engineering Meets Survival Modern restorative dentistry is no longer limited to extraction and replacement. In the era of conservative and biologically [...]
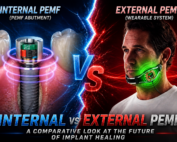
Pulsed Electromagnetic Field (PEMF) Use in Implant Dentistry
Pulsed Electromagnetic Field (PEMF) Use in Implant Dentistry Abstract and Historical Background Pulsed Electromagnetic Field (PEMF) therapy refers to the application of low-frequency electromagnetic [...]
Laser Therapy in the Management of Peri-Implantitis
Laser Therapy in the Management of Peri-Implantitis Laser technology has become an increasingly valuable adjunct in the treatment of peri-implant diseases, particularly peri-implantitis. Its [...]
Magnetically Guided Dental Nanobots (CalBots) Are Real
Magnetically Guided Dental Nanobots (CalBots) Are Real The concept of nanobots in dentistry has long been associated with futuristic speculation. However, recent peer-reviewed research [...]

Peri-Implantitis Treatment & Prevention Methods
Peri-Implantitis Treatment & Prevention Methods Peri-implantitis remains one of the most significant biological complications affecting dental implants, posing a serious threat to long-term implant [...]


{kind=link}
{kind=link}
{kind=link}