
-Around-Implants")
Coronally Advanced Flap ( CAF ): Techniques Around Implants
Coronally Advanced Flap (CAF) procedures are established in periodontal surgery for root coverage; their application around dental implants for peri-implant soft tissue dehiscences (PSTDs) has become a key technique for restoring esthetics, improving keratinized mucosa width (KMW) and mucosal thickness (MT), and protecting peri-implant health. This article reviews indications, surgical anatomy, technique variations, adjuncts, outcomes, and evidence-based recommendations for using the Coronally Advanced Flap (CAF) around implants.
Indications for Coronally Advanced Flap (CAF) around implants
Indications include isolated buccal soft tissue dehiscences over implant crowns that compromise esthetics, phonetics or hygiene access; thin peri-implant mucosa with marginal exposure after remodeling; or patient complaints of hypersensitivity/food impaction where a mucosal cover improves function. PSTDs associated with platform-switching, malpositioned implants, or inadequate buccal bone may still be treatable with CAF but require careful risk assessment—particularly when bone support is insufficient. Recent consensus highlights that CTG augmentation improves soft tissue stability when CAF is performed around implants. Nature
Pre-operative assessment and treatment planning
A specialist-level protocol should include: (1) three-dimensional evaluation of buccal bone and implant position using CBCT when indicated; (2) measurement of KMW and MT with transgingival probing or ultrasound; (3) periodontal/peri-implant infection control and prosthetic assessment (emergent overhanging margins or crown contours that traumatize tissues should be corrected before surgery). When prosthetic contours limit coronal advancement, provisional crown modification or temporary removal may be necessary. Evidence indicates soft tissue augmentation outcomes are influenced strongly by flap tension and implant position—minimizing tension is critical for predictable coverage. ScienceDirect
Surgical anatomy and biomechanics relevant to CAF
Around implants, the peri-implant mucosa differs histologically from gingiva around teeth: the absence of a periodontal ligament and different vascularity requires careful flap design to preserve blood supply. Submucosal connective tissue thickness correlates with long-term mucosal stability; therefore, a coronally advanced flap combined with connective tissue grafting (CTG) addresses both positional and thickness defects. Flap release, avoidance of vertical-release incisions when possible, and atraumatic periosteal manipulation reduce ischemic risk and fibrosis. SpringerLink
Technique: Coronally Advanced Flap (CAF) — stepwise surgical protocol
Anesthesia & incision design — Use intrasulcular incisions around the implant crown and one or two horizontal/oblique releasing incisions only if necessary; for esthetic zones, consider envelope or partial-thickness approaches to preserve papillae.
Flap elevation & tension-free release — Elevate a split-full-split or full-thickness flap to the mucogingival junction; perform careful periosteal or coronal undermining to achieve tension-free coronal positioning of the flap margin at or slightly coronal to the prosthetic CEJ.
Connective tissue graft (CTG) or substitute — Harvest palatal CTG or use xenogeneic matrix (ADM/xenograft) when CTG is contraindicated. CTG placed over the buccal aspect increases MT and improves the stability of the mucosal margin.
Stabilization — Suture the CTG if used, then coronally position the flap and secure with interrupted or sling sutures; use suturing techniques that distribute tension and avoid compromised vascularity. Tension reduction correlates with improved coverage.
Prosthetic management — Adjust provisional restorations or temporarily remove crowns when necessary to allow coronal tissue positioning and avoid pressure on the flap during healing.
Clinical trials comparing CAF + CTG with tunnel techniques around implants show that CAF + CTG achieves slightly better percentage coverage and larger gains in KMW/MT in isolated PSTDs. PubMed+1
Adjuncts and biomaterials: CTG, matrices, biologics
A CTG remains the gold standard adjunct to CAF for predictable thickness gain and stability, especially in thin biotypes. Alternatives such as acellular dermal matrices or xenogeneic collagen matrices offer less donor-site morbidity but variable long-term volumetric stability. Emerging adjuncts—concentrated growth factor (CGF), enamel matrix derivative (EMD), and platelet concentrates—have shown promising early results when combined with CAF for gingival recession and may be applied to peri-implant defects, but high-quality, long-term implant-specific data are limited. Select adjuncts based on clinician experience, patient morbidity concerns, and evidence-based outcomes. BioMed Central+1
Expected outcomes, prognosis, and complications
When properly indicated and executed, CAF around implants combined with CTG typically yields substantial recession coverage, increased KMW, and improved esthetic scores at 6–12 months; however, complete coverage is less predictable than in tooth recession cases because of implant position and bone remodeling dynamics. Complications include graft necrosis, flap dehiscence, persistent tension leading to recurrence, and esthetic mismatches between native mucosa and grafted tissue. Long-term stability depends on prosthetic contour control, absence of occlusal or biomechanical overload, patient hygiene, and smoking status. Systematic reviews show CAF + CTG as a consistently effective strategy, though heterogeneity in study designs warrants cautious interpretation. PMC+1
Practical tips for specialists to improve predictability
Minimize flap tension: aggressive periosteal release and coronal suturing strategies reduce relapse. ScienceDirect
Prefer CTG in thin biotypes: CTG confers predictable thickness gains and maintains mucosal position. Nature
Control prosthetics: reshape provisional crowns to support the new margin; avoid overcontoured crowns that press on the flap.
Smoking cessation: advise cessation pre- and post-op for at least 2–4 weeks; smoking impairs graft revascularization.
Follow up with objective measurements: KMW, MT, and photographic documentation at baseline, 3, 6, and 12 months to evaluate success and detect relapse early.
Evidence summary and clinical recommendation
High-quality randomized trials and recent systematic reviews support the use of Coronally Advanced Flap (CAF) combined with CTG as a first-line surgical approach for isolated peri-implant buccal soft tissue dehiscences when implant position and residual bone allow tissue coverage. Alternative techniques (tunneling, flapless soft tissue substitutes) are viable in selected cases, especially where donor-site morbidity is a concern or when superior esthetic blending is prioritized; however, CAF + CTG most consistently achieves greater recession coverage and KMW/MT gains in current RCTs. Individualize treatment planning based on implant position, biotype, prosthetic constraints, and patient preferences. PubMed+1
References (selected key sources)
Management of Soft Tissue Defects Around Single Implants — narrative and systematic insights. PMC. PMC
Coronally Advanced Flap versus Tunnel for Peri-Implant Soft Tissue Dehiscences — randomized clinical trial, Journal of Clinical Periodontology (2023). PubMed
Expert Consensus on Peri-Implant Keratinized Mucosa Augmentation — Nature (2025). Nature
Comparative Effectiveness of Tunneling vs. Coronally Advanced Flap — MDPI review/meta-analysis. MDPI
Concentrated Growth Factor combined with CAF — recent clinical trial (BMC Oral Health). BioMed Central
Recent Articles































Coronally Advanced Flap (CAF) procedures are established in periodontal surgery for root coverage; their application around dental implants for peri-implant soft tissue dehiscences (PSTDs) has become a key technique for restoring esthetics, improving keratinized mucosa width (KMW) and mucosal thickness (MT), and protecting peri-implant health. This article reviews indications, surgical anatomy, technique variations, adjuncts, outcomes, and evidence-based recommendations for using the Coronally Advanced Flap (CAF) around implants.
Indications for Coronally Advanced Flap (CAF) around implants
Indications include isolated buccal soft tissue dehiscences over implant crowns that compromise esthetics, phonetics or hygiene access; thin peri-implant mucosa with marginal exposure after remodeling; or patient complaints of hypersensitivity/food impaction where a mucosal cover improves function. PSTDs associated with platform-switching, malpositioned implants, or inadequate buccal bone may still be treatable with CAF but require careful risk assessment—particularly when bone support is insufficient. Recent consensus highlights that CTG augmentation improves soft tissue stability when CAF is performed around implants. Nature
Pre-operative assessment and treatment planning
A specialist-level protocol should include: (1) three-dimensional evaluation of buccal bone and implant position using CBCT when indicated; (2) measurement of KMW and MT with transgingival probing or ultrasound; (3) periodontal/peri-implant infection control and prosthetic assessment (emergent overhanging margins or crown contours that traumatize tissues should be corrected before surgery). When prosthetic contours limit coronal advancement, provisional crown modification or temporary removal may be necessary. Evidence indicates soft tissue augmentation outcomes are influenced strongly by flap tension and implant position—minimizing tension is critical for predictable coverage. ScienceDirect
Surgical anatomy and biomechanics relevant to CAF
Around implants, the peri-implant mucosa differs histologically from gingiva around teeth: the absence of a periodontal ligament and different vascularity requires careful flap design to preserve blood supply. Submucosal connective tissue thickness correlates with long-term mucosal stability; therefore, a coronally advanced flap combined with connective tissue grafting (CTG) addresses both positional and thickness defects. Flap release, avoidance of vertical-release incisions when possible, and atraumatic periosteal manipulation reduce ischemic risk and fibrosis. SpringerLink
Technique: Coronally Advanced Flap (CAF) — stepwise surgical protocol
Anesthesia & incision design — Use intrasulcular incisions around the implant crown and one or two horizontal/oblique releasing incisions only if necessary; for esthetic zones, consider envelope or partial-thickness approaches to preserve papillae.
Flap elevation & tension-free release — Elevate a split-full-split or full-thickness flap to the mucogingival junction; perform careful periosteal or coronal undermining to achieve tension-free coronal positioning of the flap margin at or slightly coronal to the prosthetic CEJ.
Connective tissue graft (CTG) or substitute — Harvest palatal CTG or use xenogeneic matrix (ADM/xenograft) when CTG is contraindicated. CTG placed over the buccal aspect increases MT and improves the stability of the mucosal margin.
Stabilization — Suture the CTG if used, then coronally position the flap and secure with interrupted or sling sutures; use suturing techniques that distribute tension and avoid compromised vascularity. Tension reduction correlates with improved coverage.
Prosthetic management — Adjust provisional restorations or temporarily remove crowns when necessary to allow coronal tissue positioning and avoid pressure on the flap during healing.
Clinical trials comparing CAF + CTG with tunnel techniques around implants show that CAF + CTG achieves slightly better percentage coverage and larger gains in KMW/MT in isolated PSTDs. PubMed+1
Adjuncts and biomaterials: CTG, matrices, biologics
A CTG remains the gold standard adjunct to CAF for predictable thickness gain and stability, especially in thin biotypes. Alternatives such as acellular dermal matrices or xenogeneic collagen matrices offer less donor-site morbidity but variable long-term volumetric stability. Emerging adjuncts—concentrated growth factor (CGF), enamel matrix derivative (EMD), and platelet concentrates—have shown promising early results when combined with CAF for gingival recession and may be applied to peri-implant defects, but high-quality, long-term implant-specific data are limited. Select adjuncts based on clinician experience, patient morbidity concerns, and evidence-based outcomes. BioMed Central+1
Expected outcomes, prognosis, and complications
When properly indicated and executed, CAF around implants combined with CTG typically yields substantial recession coverage, increased KMW, and improved esthetic scores at 6–12 months; however, complete coverage is less predictable than in tooth recession cases because of implant position and bone remodeling dynamics. Complications include graft necrosis, flap dehiscence, persistent tension leading to recurrence, and esthetic mismatches between native mucosa and grafted tissue. Long-term stability depends on prosthetic contour control, absence of occlusal or biomechanical overload, patient hygiene, and smoking status. Systematic reviews show CAF + CTG as a consistently effective strategy, though heterogeneity in study designs warrants cautious interpretation. PMC+1
Practical tips for specialists to improve predictability
Minimize flap tension: aggressive periosteal release and coronal suturing strategies reduce relapse. ScienceDirect
Prefer CTG in thin biotypes: CTG confers predictable thickness gains and maintains mucosal position. Nature
Control prosthetics: reshape provisional crowns to support the new margin; avoid overcontoured crowns that press on the flap.
Smoking cessation: advise cessation pre- and post-op for at least 2–4 weeks; smoking impairs graft revascularization.
Follow up with objective measurements: KMW, MT, and photographic documentation at baseline, 3, 6, and 12 months to evaluate success and detect relapse early.
Evidence summary and clinical recommendation
High-quality randomized trials and recent systematic reviews support the use of Coronally Advanced Flap (CAF) combined with CTG as a first-line surgical approach for isolated peri-implant buccal soft tissue dehiscences when implant position and residual bone allow tissue coverage. Alternative techniques (tunneling, flapless soft tissue substitutes) are viable in selected cases, especially where donor-site morbidity is a concern or when superior esthetic blending is prioritized; however, CAF + CTG most consistently achieves greater recession coverage and KMW/MT gains in current RCTs. Individualize treatment planning based on implant position, biotype, prosthetic constraints, and patient preferences. PubMed+1
References (selected key sources)
Management of Soft Tissue Defects Around Single Implants — narrative and systematic insights. PMC. PMC
Coronally Advanced Flap versus Tunnel for Peri-Implant Soft Tissue Dehiscences — randomized clinical trial, Journal of Clinical Periodontology (2023). PubMed
Expert Consensus on Peri-Implant Keratinized Mucosa Augmentation — Nature (2025). Nature
Comparative Effectiveness of Tunneling vs. Coronally Advanced Flap — MDPI review/meta-analysis. MDPI
Concentrated Growth Factor combined with CAF — recent clinical trial (BMC Oral Health). BioMed Central
Recent Articles
Magnetically Guided Dental Nanobots (CalBots) Are Real
Magnetically Guided Dental Nanobots (CalBots) Are Real The concept of nanobots in dentistry has long been associated with futuristic speculation. However, recent peer-reviewed research [...]

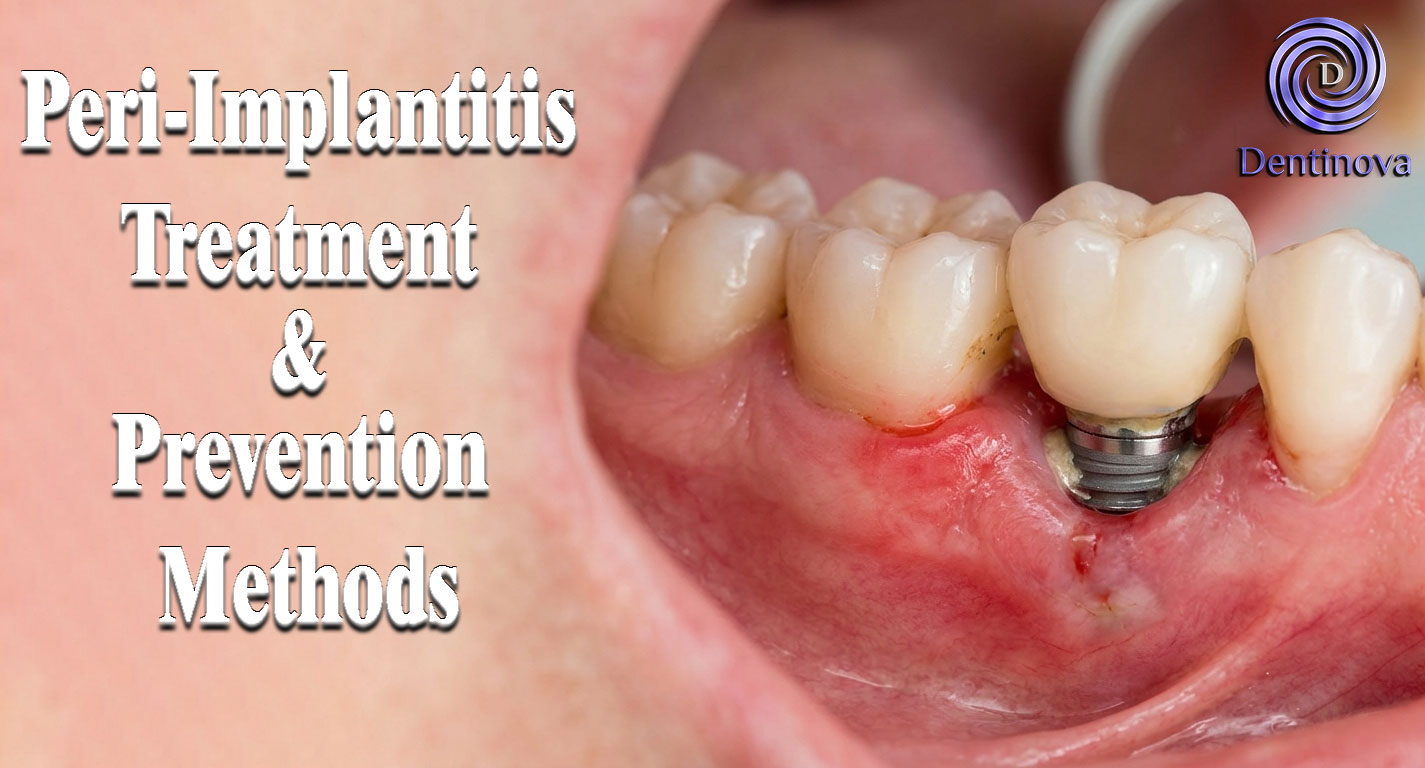
Peri-Implantitis Treatment & Prevention Methods
Peri-Implantitis Treatment & Prevention Methods Peri-implantitis remains one of the most significant biological complications affecting dental implants, posing a serious threat to long-term implant [...]
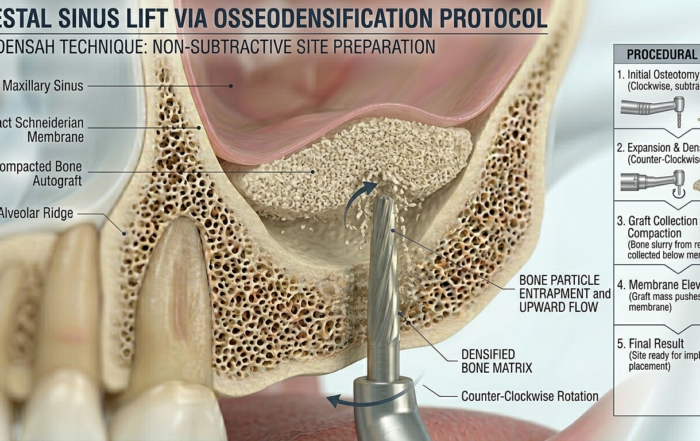
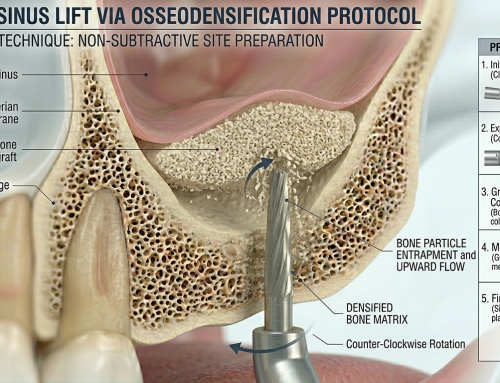
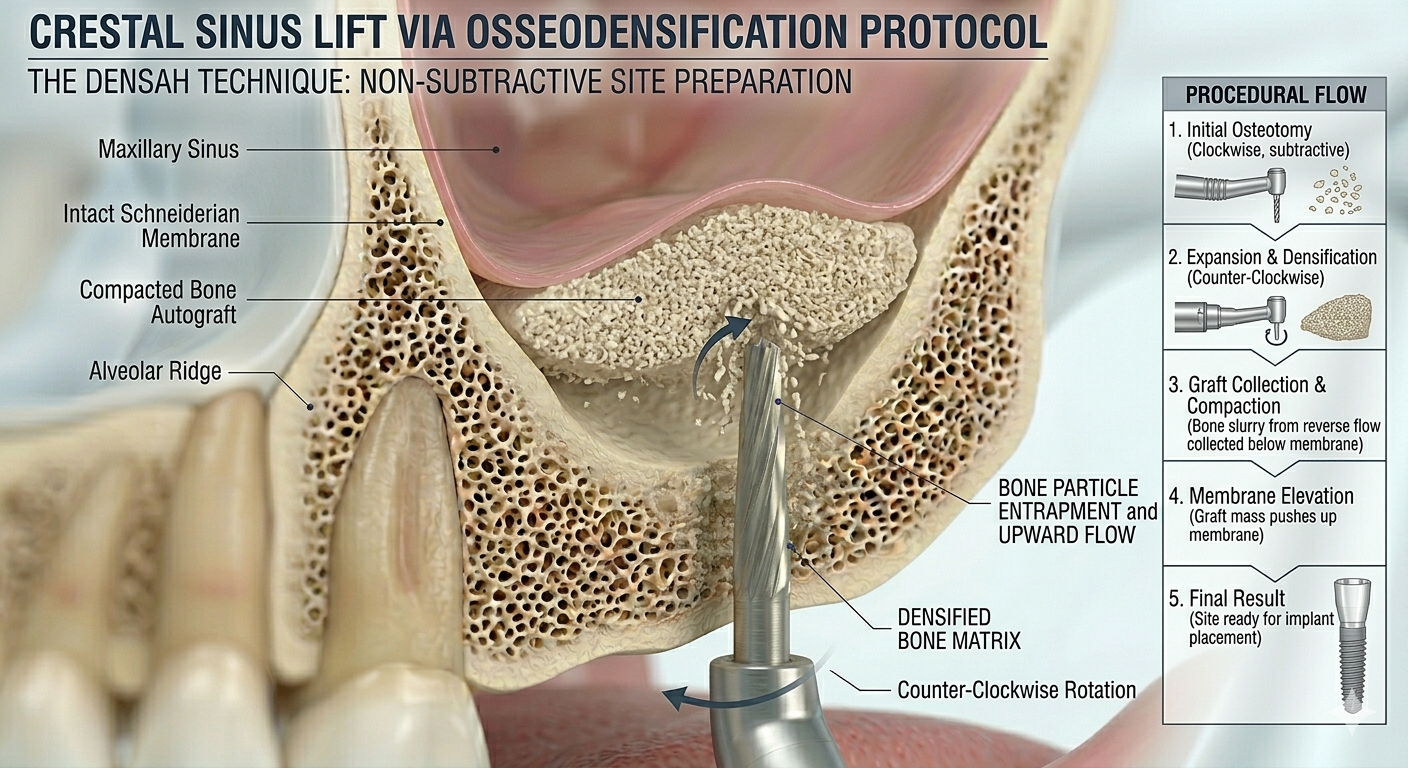
Latest Sinus Lifting Techniques in Modern Implant Dentistry
Latest Sinus Lifting Techniques in Modern Implant Dentistry A Comprehensive Clinical Review Introduction to Sinus Lifting in Implantology Sinus lifting, or maxillary sinus floor [...]

Biomechanics of the Triple Abutment & BOPiT Concept
Dental Biomechanics · Implant Science · Clinical Evidence Biomechanics of the Triple Abutment & BOPiT Concept How a saddle-shaped mathematical surface is rewriting the rules of load distribution [...]

The Woman Who Proved One Implant Could Hold Three Crowns
The Woman Who Proved One Implant Could Hold Three Crowns While the dental establishment looked away, Dr. Luciana Colepícolo spent 12 years building the [...]
ENPP1, The Molecular Brake That Limits Tissue Healing
ENPP1, The Molecular Brake That Limits Tissue Healing Introduction: A New Biological Barrier to Dental Regeneration Meet ENPP1—a protein most dentists have never heard [...]






{kind=link}
{kind=link}
{kind=link}