

True vs. Pseudo Tug-back in Root Canal Obturation
In endodontics, achieving a high-quality apical seal is fundamental to the long-term success of root canal treatment. One of the most widely used indicators of proper apical fit before obturation is the concept of tug-back. While many clinicians are trained to look for adequate resistance when pulling on the master gutta-percha (GP) cone, not all forms of tug-back reflect true apical adaptation. In fact, misunderstanding this concept can lead to pseudo tug-back, a deceptive clinical sign that compromises the apical seal and increases the risk of postoperative complications. This article explains the difference between true and pseudo tug-back, how to identify each, and practical clinical steps to ensure a predictable apical fit.
Understanding the Concept of True Tug-back
True tug-back refers to the gentle resistance felt when withdrawing a master GP cone that fits snugly at the apical third of the root canal. This sensation indicates that the shape of the prepared canal closely matches the shape and taper of the GP cone. When true tug-back is present, the clinician can be confident that the cone is binding specifically at the apex, where a fluid-tight seal is required to prevent bacterial penetration.
Achieving true tug-back offers several endodontic advantages. First, it enhances the quality of the apical seal, reducing the risk of microleakage and reinfection. Second, it ensures that the GP cone matches the canal geometry, improving the adaptation of the sealer during obturation. Third, it prevents the extrusion of gutta-percha during warm vertical compaction, a complication that occurs when the cone is not properly anchored at the apex. Thus, true tug-back is not merely a tactile preference but a scientific indicator of three-dimensional canal obturation quality.
Pseudo Tug-back: A Common but Misleading Clinical Pitfall
Pseudo tug-back occurs when the master GP cone exhibits resistance upon withdrawal, but the binding does not occur at the apical third. Instead, it results from friction or binding in the mid or coronal third of the canal. This is typically due to a mismatch in taper between the canal preparation and the GP cone. The cone may feel “tight,” yet it fails to engage the apical constriction. This false sense of security contributes to poor apical sealing and can compromise the entire obturation.
The primary cause of pseudo tug-back is inadequate canal shaping—specifically when the file taper does not match the cone taper. For example, a canal prepared with insufficient mid- and coronal flaring allows the GP cone to wedge coronally, creating the illusion of tug-back. Clinically, this is dangerous because the apex remains unsealed, and warm vertical condensation may drive GP beyond the apical foramen due to a lack of apical resistance. Identifying pseudo tug-back, therefore, is crucial for avoiding obturation failures.
How to Identify True vs. Pseudo Tug-back
A reliable method for distinguishing true from false tug-back begins with a well-prepared and thoroughly cleaned root canal system. The master cone trial should always be performed with a moist canal environment, as this simulates the presence of sealer during final obturation.
After gently inserting the master cone to working length, the clinician should remove it and examine the surface under magnification. True tug-back produces crimping marks or slight indentations on the apical segment of the cone. These marks show where the cone binds against the apical third of the canal. In contrast, pseudo tug-back produces crimping along the mid or coronal third, indicating that the cone is wedging coronally rather than fitting apically.
Radiographic verification is also essential. A properly fitted cone should show close adaptation at the apical third with no visible radiolucent spaces. If radiographs reveal spacing apically but tightness coronally, pseudo tug-back is likely present.
Clinical Strategies for Achieving Reliable Apical Fit
When true tug-back is absent, several corrective measures can be implemented. If coronally or mid-root binding occurs, additional flaring with brushing strokes directed away from the furcation may be necessary. This ensures the canal taper progresses smoothly toward the apex, allowing the GP cone to seat correctly.
If the cone reaches full working length yet shows no apical tug-back, trimming 0.5 mm from the apical end of the cone may improve apical adaptation. Alternatively, apical gauging using hand files helps determine whether the apical preparation is adequate for the selected cone size.
For challenging canal anatomies, clinicians may choose fitted or Auto-Fit GP cones that can be trimmed precisely to length. These cones are especially useful with warm vertical condensation techniques, where precise apical engagement is essential for preventing extrusion.
Pseudo Tug-back and Its Impact on Obturation Quality
Pseudo tug-back significantly compromises obturation quality by leaving the apical third inadequately sealed. Without proper apical binding, sealer extrusion becomes more likely, and GP may not compact properly within the canal. Bacterial ingress into the apical area becomes a long-term risk, potentially leading to persistent periapical inflammation.
Furthermore, false tug-back creates unpredictability in the obturation process. During warm vertical condensation, downward pressure may push softened GP beyond the foramen, causing postoperative pain or delayed healing. Therefore, recognizing and correcting pseudo tug-back is essential for predictable, long-term clinical success.
Ensuring Predictable Outcomes in Root Canal Obturation
Clinicians can ensure consistent results by standardizing their canal preparation, using cone-fit radiographs, and practicing routine cone surface inspection under magnification. Additionally, selecting GP cones that match the exact taper and size of the final shaping instrument greatly increases the likelihood of true tug-back. Continued education and understanding of canal morphology also play major roles in preventing pseudo tug-back and refining obturation techniques.
References
- Schilder H. Filling root canals in three dimensions. Dent Clin North Am. 1967.
- Gu LS, Ling JQ, et al. Apical sealing ability of different obturation techniques. J Endod. Various editions.
FAQ
1. What is tug-back in endodontics?
Tug-back is the resistance felt when removing a master GP cone that fits properly in the apical third of the canal. It indicates good apical adaptation before obturation.
2. How can I differentiate true from pseudo tug-back?
Inspect the cone for apical crimping marks and verify with a radiograph. True tug-back shows apical binding; pseudo tug-back shows mid or coronal binding.
3. What causes pseudo tug-back?
Mismatch between canal taper and GP cone taper, inadequate coronal flaring, or improper shaping leads to mid-coronal binding instead of apical adaptation.
4. Can pseudo tug-back affect the apical seal?
Yes. Because the cone does not bind apically, the seal is compromised, increasing the risk of bacterial leakage and postoperative issues.
5. What should I do if the master cone doesn’t show true tug-back?
Try apical gauging, trimming the cone by 0.5 mm, performing additional coronal/mid-root flaring, or using fitted/Auto-Fit GP cones for precise adaptation.
Recent Articles



































In endodontics, achieving a high-quality apical seal is fundamental to the long-term success of root canal treatment. One of the most widely used indicators of proper apical fit before obturation is the concept of tug-back. While many clinicians are trained to look for adequate resistance when pulling on the master gutta-percha (GP) cone, not all forms of tug-back reflect true apical adaptation. In fact, misunderstanding this concept can lead to pseudo tug-back, a deceptive clinical sign that compromises the apical seal and increases the risk of postoperative complications. This article explains the difference between true and pseudo tug-back, how to identify each, and practical clinical steps to ensure a predictable apical fit.
Understanding the Concept of True Tug-back
True tug-back refers to the gentle resistance felt when withdrawing a master GP cone that fits snugly at the apical third of the root canal. This sensation indicates that the shape of the prepared canal closely matches the shape and taper of the GP cone. When true tug-back is present, the clinician can be confident that the cone is binding specifically at the apex, where a fluid-tight seal is required to prevent bacterial penetration.
Achieving true tug-back offers several endodontic advantages. First, it enhances the quality of the apical seal, reducing the risk of microleakage and reinfection. Second, it ensures that the GP cone matches the canal geometry, improving the adaptation of the sealer during obturation. Third, it prevents the extrusion of gutta-percha during warm vertical compaction, a complication that occurs when the cone is not properly anchored at the apex. Thus, true tug-back is not merely a tactile preference but a scientific indicator of three-dimensional canal obturation quality.
Pseudo Tug-back: A Common but Misleading Clinical Pitfall
Pseudo tug-back occurs when the master GP cone exhibits resistance upon withdrawal, but the binding does not occur at the apical third. Instead, it results from friction or binding in the mid or coronal third of the canal. This is typically due to a mismatch in taper between the canal preparation and the GP cone. The cone may feel “tight,” yet it fails to engage the apical constriction. This false sense of security contributes to poor apical sealing and can compromise the entire obturation.
The primary cause of pseudo tug-back is inadequate canal shaping—specifically when the file taper does not match the cone taper. For example, a canal prepared with insufficient mid- and coronal flaring allows the GP cone to wedge coronally, creating the illusion of tug-back. Clinically, this is dangerous because the apex remains unsealed, and warm vertical condensation may drive GP beyond the apical foramen due to a lack of apical resistance. Identifying pseudo tug-back, therefore, is crucial for avoiding obturation failures.
How to Identify True vs. Pseudo Tug-back
A reliable method for distinguishing true from false tug-back begins with a well-prepared and thoroughly cleaned root canal system. The master cone trial should always be performed with a moist canal environment, as this simulates the presence of sealer during final obturation.
After gently inserting the master cone to working length, the clinician should remove it and examine the surface under magnification. True tug-back produces crimping marks or slight indentations on the apical segment of the cone. These marks show where the cone binds against the apical third of the canal. In contrast, pseudo tug-back produces crimping along the mid or coronal third, indicating that the cone is wedging coronally rather than fitting apically.
Radiographic verification is also essential. A properly fitted cone should show close adaptation at the apical third with no visible radiolucent spaces. If radiographs reveal spacing apically but tightness coronally, pseudo tug-back is likely present.
Clinical Strategies for Achieving Reliable Apical Fit
When true tug-back is absent, several corrective measures can be implemented. If coronally or mid-root binding occurs, additional flaring with brushing strokes directed away from the furcation may be necessary. This ensures the canal taper progresses smoothly toward the apex, allowing the GP cone to seat correctly.
If the cone reaches full working length yet shows no apical tug-back, trimming 0.5 mm from the apical end of the cone may improve apical adaptation. Alternatively, apical gauging using hand files helps determine whether the apical preparation is adequate for the selected cone size.
For challenging canal anatomies, clinicians may choose fitted or Auto-Fit GP cones that can be trimmed precisely to length. These cones are especially useful with warm vertical condensation techniques, where precise apical engagement is essential for preventing extrusion.
Pseudo Tug-back and Its Impact on Obturation Quality
Pseudo tug-back significantly compromises obturation quality by leaving the apical third inadequately sealed. Without proper apical binding, sealer extrusion becomes more likely, and GP may not compact properly within the canal. Bacterial ingress into the apical area becomes a long-term risk, potentially leading to persistent periapical inflammation.
Furthermore, false tug-back creates unpredictability in the obturation process. During warm vertical condensation, downward pressure may push softened GP beyond the foramen, causing postoperative pain or delayed healing. Therefore, recognizing and correcting pseudo tug-back is essential for predictable, long-term clinical success.
Ensuring Predictable Outcomes in Root Canal Obturation
Clinicians can ensure consistent results by standardizing their canal preparation, using cone-fit radiographs, and practicing routine cone surface inspection under magnification. Additionally, selecting GP cones that match the exact taper and size of the final shaping instrument greatly increases the likelihood of true tug-back. Continued education and understanding of canal morphology also play major roles in preventing pseudo tug-back and refining obturation techniques.
References
- Schilder H. Filling root canals in three dimensions. Dent Clin North Am. 1967.
- Gu LS, Ling JQ, et al. Apical sealing ability of different obturation techniques. J Endod. Various editions.
FAQ
1. What is tug-back in endodontics?
Tug-back is the resistance felt when removing a master GP cone that fits properly in the apical third of the canal. It indicates good apical adaptation before obturation.
2. How can I differentiate true from pseudo tug-back?
Inspect the cone for apical crimping marks and verify with a radiograph. True tug-back shows apical binding; pseudo tug-back shows mid or coronal binding.
3. What causes pseudo tug-back?
Mismatch between canal taper and GP cone taper, inadequate coronal flaring, or improper shaping leads to mid-coronal binding instead of apical adaptation.
4. Can pseudo tug-back affect the apical seal?
Yes. Because the cone does not bind apically, the seal is compromised, increasing the risk of bacterial leakage and postoperative issues.
5. What should I do if the master cone doesn’t show true tug-back?
Try apical gauging, trimming the cone by 0.5 mm, performing additional coronal/mid-root flaring, or using fitted/Auto-Fit GP cones for precise adaptation.
Recent Articles

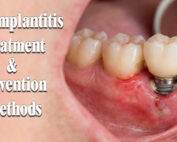
Peri-Implantitis Treatment & Prevention Methods
Peri-Implantitis Treatment & Prevention Methods Peri-implantitis remains one of the most significant biological complications affecting dental implants, posing a serious threat to long-term implant [...]
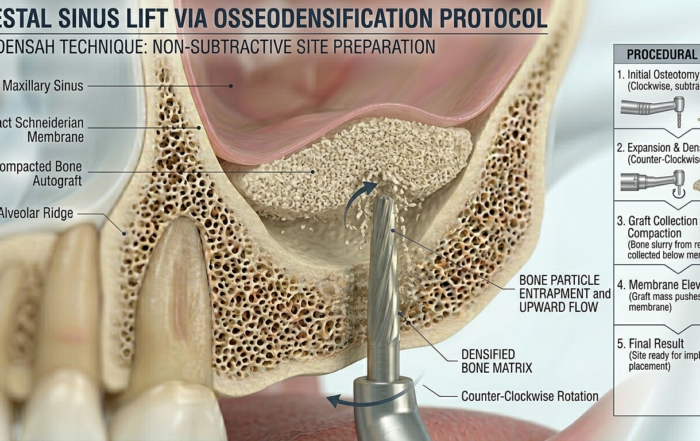
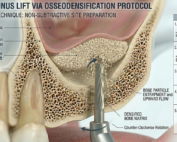
Latest Sinus Lifting Techniques in Modern Implant Dentistry
Latest Sinus Lifting Techniques in Modern Implant Dentistry A Comprehensive Clinical Review Introduction to Sinus Lifting in Implantology Sinus lifting, or maxillary sinus floor [...]

Biomechanics of the Triple Abutment & BOPiT Concept
Dental Biomechanics · Implant Science · Clinical Evidence Biomechanics of the Triple Abutment & BOPiT Concept How a saddle-shaped mathematical surface is rewriting the rules of load distribution [...]

The Woman Who Proved One Implant Could Hold Three Crowns
The Woman Who Proved One Implant Could Hold Three Crowns While the dental establishment looked away, Dr. Luciana Colepícolo spent 12 years building the [...]
ENPP1, The Molecular Brake That Limits Tissue Healing
ENPP1, The Molecular Brake That Limits Tissue Healing Introduction: A New Biological Barrier to Dental Regeneration Meet ENPP1—a protein most dentists have never heard [...]
The Rise of Self‑Healing Dental Biomaterials
The Rise of Self‑Healing Dental Biomaterials Introduction In modern restorative dentistry, durability and longevity of materials remain among the greatest clinical challenges. Traditional dental [...]


{kind=link}
{kind=link}
{kind=link}